
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
A case report of a rare mesenteric lesion
Clotylde Dumas; Anna Wolski; Marie Pascal; Diane Mege*
Aix Marseille Univ, APHM, Department of Digestive Surgery, Timone University, Marseille, France.
*Corresponding Author : Diane Mege
Aix Marseille Univ, APHM, Department of Digestive Surgery, Timone University Hospital, 264 rue Saint-Pierre, 13005, Marseille, France.
Tel: +33491388487, Fax: +33491385355;
Email: dr.dianemege@gmail.com
Received : Oct 23, 2023
Accepted : Nov 21, 2023
Published : Nov 28, 2023
Archived : www.jcimcr.org
Copyright : © Mege D (2023).
Keywords: Lymphangioma; Abdominal lymphangioma; Cystic mesenteric lesion; Heterogenous mesenteric mass.
Citation: Dumas C, Wolski A, Pascal M, Mege D. A case report of a rare mesenteric lesion. J Clin Images Med Case Rep. 2023; 4(11): 2708.
Description
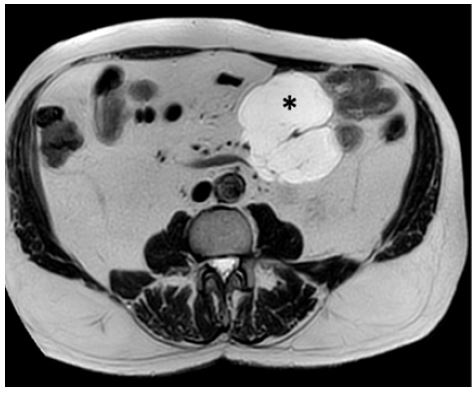
In a 82-year-old man with cardiovascular comorbidities underwent an abdominal CT scan, showing an incidental 9 centimeters cystic mesenteric lesion. An additional Magnetic Resonance Imaging (MRI) described a not-enhanced cystic lesion, with septa, developed in the mesenteric root with a mass effect without any sign of bowel invasion (Figure 1). This lesion was not observed in a previous abdominal CT scan. A cystic peritoneal mesothelium was suspected. A surgical treatment was thus indicated. Because of the location at the mesenteric root, an open approach was performed, revealing a cystic mesenteric multi-loculated lesion, with white liquid contain (Figure 2). A bowel resection of proximal jejunum (45 centimeters) was performed with an handsewn end-to-end anastomosis. Pathological analysis identified a cystic mesenteric lymphangioma without any criteria of malignity.
Cystic lymphangioma is a rare benign tumor with ectopic lymphatic vessels, most common in children. Cervico-facial location is the most frequent, in 60% of cases. Profound abdomiabdominal location is rare, between 2 and 10% of cases, with an incidence of 1/100000 adults and 1/20000 children per year [1]. In this location, patients are usually not symptomatic, but the lesion grows considerably and can induce a clinical mass effect. Management of these lesions is based on follow-up, surgical resection [2], or intra-cystic injection of sclerotic drug in the case of unresectable lesions [3]. Recurrence is frequent and depends on the surgical resection.

Statements and declarations
Conflict of interest disclosure: None.
Funding statement: None.
Ethics approval statement: Not necessary.
Patient consent statement: Yes.
References
- Chegdali O, Guedira M, Benaddi L, El Idrissi Lamghari A, Lachkar H, et al. Cystic abdominal lymphangioma in adult. Acta Endoscopica. 2004; 34: 245-248.
- Sana L, Fehd K, Imen R, Faouzi C. Mesenteric cystic lymphangioma. Surgery. 2021; 170: e25-6.
- Bezzola T, Bühler L, Chardot C, Morel P. Surgical therapy of abdominal cystic lymphangioma in adults and children. Journal of Surgery. 2008; 145: 238-243.