
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Mitral valve endocarditis presenting as a stroke in a young lady: A case report
Malagalage Nishadi Saumya Kumari Perer1*; Aruna Gunapala2
1Senior Registrar, Internal Medicine, National Hospital of Sri Lanka, Sri Lanka.
2Consultant Physician, National Hospital of Sri Lanka, Sri Lanka.
*Corresponding Author : Malagalage Nishadi Saumya Kumari Perera
Senior Registrar, Internal Medicine, National Hospital of Sri Lanka, Sri Lanka.
Email: nishadiperera19@yahoo.com
Received : Oct 21, 2023
Accepted : Nov 21, 2023
Published : Nov 28, 2023
Archived : www.jcimcr.org
Copyright : © Kumari Perer MNS (2023).
Abstract
Left-sided infective endocarditis is a recognized but less common cause of cerebral embolism. When the causative organism is Methicillin- resistant Staphylococcus aureus, the rate of embolic phenomena increases. In such cases, surgical interventions should be considered when indicated.
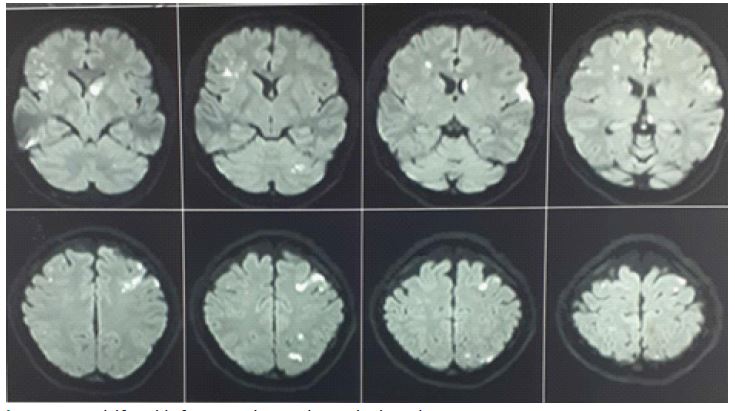
We present a case of a 20-year-old girl who presented with acute onset aphasia, and found to be having multifocal acute cerebral infarctions in brain imaging, which do not fall into a single vascular territory. Her echocardiogram confirmed mitral valve endocarditis while blood cultures were positive for Methicillin- resistant Staphylococcus aureus. She responded poorly to antibiotics and ultimately ended up with metallic prosthetic mitral valve replacement.
Keywords: Infective endocarditis; Mitral valve; Methicillin resistant; Staphylococcus aureus.
Citation: Kumari Perer MNS, Gunapala A. Mitral valve endocarditis presenting as a stroke in a young lady: A case report. J Clin Images Med Case Rep. 2023; 4(11): 2709.
Introduction
Native valve endocarditis with Methicillin-resistant Staphylococcus aureus is a condition with high morbidity and mortality. Appropriate and timely surgical interventions coupled with proper antibiotic management give successful results even if the course is complicated with embolic phenomena.
Case presentation
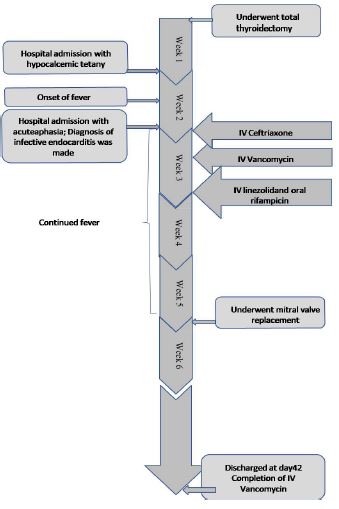
A 20-year-old girl, a known patient with papillary carcinoma of the thyroid, presented with a sudden onset inability to speak. She underwent total thyroidectomy 2 weeks prior to the presentation. She had a hospital admission 1 week after the surgery with tetany, where she was managed inward, with intravenous calcium.
On the day of the current presentation, she suddenly lost her ability to express herself. Three days prior to the disability she was having low-grade fever, which was treated with oral co-amoxiclav by the primary care physician, for a presumed lower urinary tract infection. However, fever didn’t subside and, instead worsened with chills on the day of admission. She didn’t notice any limb weakness, postural imbalance, vertigo, facial drooping or difficulty in swallowing. However, just prior to admission, she had one episode of vomiting. She didn’t have headache or seizures.
On clinical examination, she was febrile and pale, not icteric, not noted to have clubbing or oedema. She had Osler’s nodes in fingers and Janeway lesions in soles.
She had expressive aphasia, but rest of her higher functions were intact. Cranial nerve examination was normal except for a mild left ear sensorineural hearing deafness. Fundi were normal. There were no cerebellar signs. Limb examination was normal. Her pulse was of good volume and regular with a rate of 110 per minute. All the peripheral pulses were palpable. Jugular venous pulse was not elevated. Blood pressure was 120/80 mmHg. There were no carotid bruits. First and second heart sounds were normal; and there was a pan systolic murmur best heard at the apex, which was consistent with a new mitral regurgitation. Lungs had vesicular breath sounds without added sounds. Her abdominal examination was unremarkable. She was clinically euthyroid; there were no clinical features of hypocalcaemia.
Table 1: Investigations.
WBC: White Blood Cells; N%: Neutrophils percentage; L%: Lymphocyte percentage; MCV: Mean Corpuscular Volume; CRP: C Reactive Protein; ESR: Erythrocyte Sedimentation Rate; INR: International Normalized Ratio; PT: Prothrombin Time; APTT: Activated partial Thromboplastin Time; TSH: Thyroid stimulatory hormone.
Her basic investigations are summarized in table 1.
She underwent urgent Magnetic Resonance Imaging (MRI) of brain, which revealed multifocal acute cerebral infarctions which do not fall into a single vascular territory (Figure 1).
Electrocardiogram showed sinus tachycardia. Cardiac biomarkers were negative.
Chest X ray didn’t show evidence of cardiac failure.
Echocardiography findings were:
Transthoracic echocardiogram
Ventricular and atrial sizes- normal Left ventricular ejection fraction-60% Posterior mitral valvular mass.
Transoesophageal echocardiogram
Large frond like vegetation attached to base of posterior mitral valve leaflet; size 20×4 mm, with perforation in posterior mitral valve leaflet. Moderate to severe mitral regurgitation Left atrium was free of clots aortic valve was normal mild tricuspid regurgitation normal pulmonary venous drainage.
In the meantime, her blood culture yielded Methicillin-resistant Staphylococcus aureus which was sensitive to teicoplanin, vancomycin, linezolid and rifampicin, but resistant to flucloxacillin and cloxacillin.
She was managed as mitral valve endocarditis due to Methicillin-resistant Staphylococcus aureus infection, complicated with septic cerebral emboli. Her aphasia recovered within 24 hours from onset, and there was no development of new neurological weaknesses.
She was initially started on intravenous ceftriaxone, pending the blood culture results, later converted to intravenous vancomycin. Repeated blood cultures after commencement of vancomycin remained positive, so intravenous linezolid and oral rifampicin were added. However, her fever spikes persisted without much clinical response after 2 weeks of antibiotic continuation. At her third week of illness, she underwent metallic prosthetic mitral valve replacement surgery. Intraoperative finding was a large vegetation attached to posterior mitral valve leaflet with destruction of the posterior mitral valve leaflet.
She made a satisfactory clinical recovery with settling of fever following surgery. Intravenous vancomycin was continued until 42 days completion, linezolid until 21 days completion and oral rifampicin until 14 days completion. Post-operative echocardiogram demonstrated functioning prosthetic valve, without peri-valvular leak. Other valves were normal and there were no pericardial effusions.
Warfarin was started to continue lifelong, with a target INR of 2.5 to 3.5. Patient was given a proper plan on indications for antibiotic prophylaxis following the prosthetic valve replacement. Thyroxine 175 microgram was continued with monitoring of TSH. Oral calcium and vitamin D supplements were continued. She is currently doing well, under medical unit; cardiology unit and cardiothoracic unit follow up.
Discussion
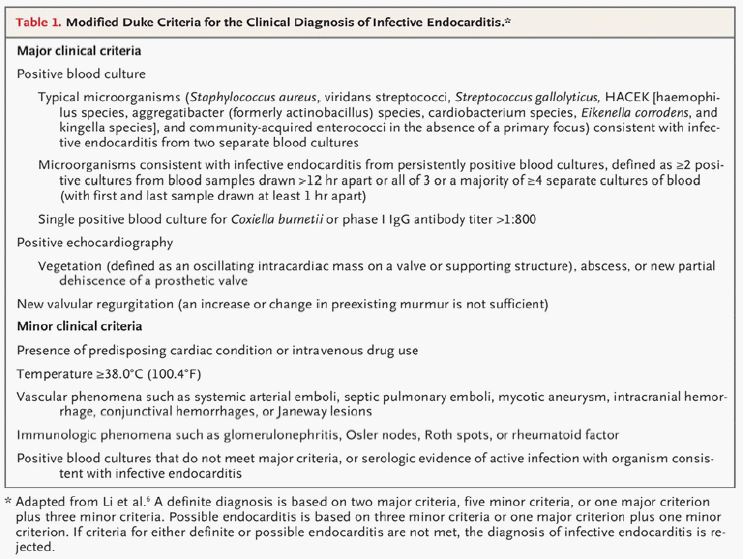
This patient who underwent several hospital admissions and received intravenous medications, came with fever followed by sudden neurological weakness manifested as aphasia. At the same time, neuroimaging was convincing of an embolic phenomenon due to involvement of multiple vascular territories. Her echocardiogram confirmed the presence of mitral valve vegetation, while the causative organism was yielded in blood cultures. She had other supportive evidence such as neutrophil leucocytosis and raised inflammatory markers. At the same time, there were other immunological manifestations of endocarditis including Osler’s nodes, all contributing to fulfil Duke’s criteria for diagnosis of infective endocarditis.
Usual presentation of majority of endocarditis patients include fever, features of septicaemia and cardiac symptoms. Neurological manifestations rarely can be the presenting symptom, or can be apparent during the course of the illness [2]. Septic embolization from the infected left sided valves, leading to stroke is a recognized complication of endocarditis. In 50% of patients with left sided endocarditis, septic cerebral embolization occurs, while clinical manifestations occur in 10-30% of patients only [3]. So, majority can remain silent and can be detected by neuroimaging only. Emboli are usually bilateral, multiple and can involve multiple arterial territories in brain [4].
Other than presentation with stroke or transient ischaemic attack due to vaso-occlusion, they can get cerebral abscesses, mycotic aneurysms and intracranial haemorrhages as neurological complications [5]. When the presentation was with neurological sequalae mimicking stroke, it is prudent to diagnose infective endocarditis as the causative pathology correctly, because it is a contraindication for thrombolysis [6].
Among the common organisms responsible for native valve endocarditis, Staphylococcus aureus is becoming more reported lately, when compared to the coagulase negative organisms [7]. At the same time, methicillin resistant strains are reported as health care associated infective endocarditis, due to wide usage of intravenous catheters and devices [8]. This patient’s clinical presentation preceded by 2 recent hospital admissions, one for total thyroidectomy and the second for management of tetany. During both occasions, she has had intravenous access which were presumed to have contributed as portal of entry of the organism. Staphylococcus aureus related endocarditis is associated with higher morbidity including increased rates of embolic phenomena and increased mortality [8].
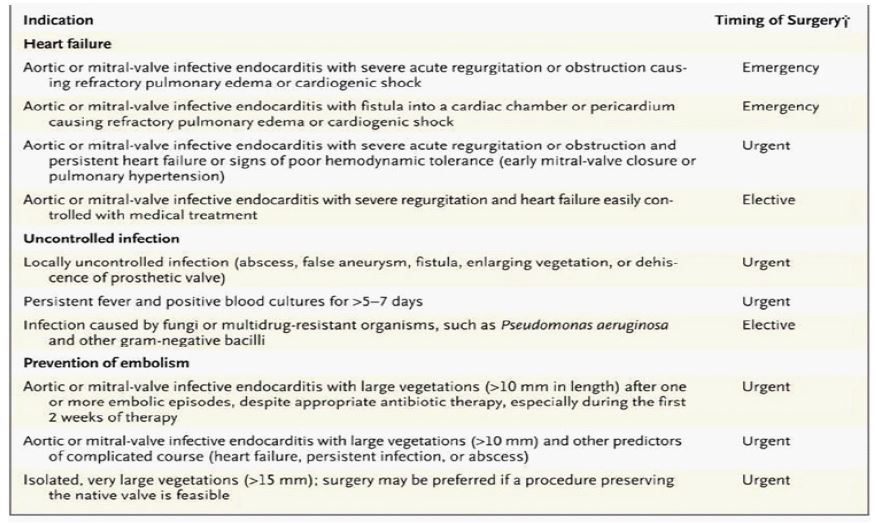
This patient’s fever didn’t subside even at the 2nd week of optimal antibiotics treatment according to the culture and sensitivity pattern. At the end of 1 week of antibiotic course, blood cultures remained positive for the same organism. At the same time, the mitral valve vegetation size was >10 mm, with embolic phenomena.
Above features indicate uncontrolled infection and liability to undergo embolism, which itself are indications to consider surgical management on urgent basis.
This patient underwent surgery at her 3rd week of illness. Intra-operative findings were compatible with extensive destruction of the mitral valve which necessitated mitral valve replacement rather than a repair. Early surgical interventions prevented her progressing into cardiac failure or further embolic phenomena.
Her story illustrates a case of native valve endocarditis from a highly virulent organism, which presented with rare cerebral embolic phenomena. Though her clinical course was complicated with uncontrolled infection, appropriate and timely surgical interventions bridged with appropriate antibiotic regimen led to a successful outcome.
Acknowledgment: We would like to thank the patient who gave us her support during the ward stay and upon preparing the case study.
Ethical considerations: This case report and its preparation adhered to international standard ethical principles. Authors have no conflicts of interest to declare.
References
- Chambers HF, Bayer AS. Native-Valve Infective Endocarditis. N Engl J Med. 2020; 383: 567-576.
- Baddour LM, Wilson WR, Bayer AS, Fowler VG, Bolger AF, et al. Infective endocarditis: Diagnosis, antimicrobial therapy, and management of complications: A statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association. Circulation. 2005; 111: e394-434.
- Keynan Y, Rubinstein E. Pathophysiology of Infective Endocarditis. Curr Infect Dis Rep. 2013; 15: 342-3463
- Sonneville R, Mirabel M, Hajage D, Tubach F, Vignon P, et al. Neurologic complications and outcomes of infective endocarditis in critically ill patients: The ENDOcardite en RE Animation prospective multicenter study. Crit Care Med. 2011; 39: 1474-81.
- Grecu N, et al. Endocarditis and stroke MAEDICA- a Journal of Clinical Medicine. 2014; 9: 375-381
- Furie KL, Jayaraman MV. 2018 guidelines for the early management of patients with acute ischemic stroke. Stroke. 2018; 49: 509-510.
- Tleyjeh IM, Steckelberg JM, Murad HS, et al. Temporal trends in infective endocarditis: A population-based study in Olmsted County, Minnesota. JAMA. 2005; 293: 3061-2.
- Miro JM, Anguera I, Cabell CH, et al. Staphylococcus aureus native valve infective endocarditis: Report of 566 episodes from the International Collaboration on Endocarditis Merged Database. Clin Infect Dis. 2005; 41: 507-51.