
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Commentary - Open Access, Volume 4
Kurt Schwitters´ medical biography: Health problems and impact on creativity
Henning Zeidler1*; Gwendolen Webster2
1Medical School Hannover, Germany.
2Founding President Kurt Schwitters Society, United Kingdom.
*Corresponding Author : Henning Zeidler
Medical School Hannover Carl-Neuberg-Str. 1 30625 Hannover.
Email: zeidler.henning@mh-hannover.de
Received : Oct 28, 2023
Accepted : Nov 22, 2023
Published : Nov 29, 2023
Archived : www.jcimcr.org
Copyright : © Zeidler H (2023).
Abstract
Kurt Schwitters (born June 20, 1887 in Hannover, † January 8, 1948 in Kendal, Cumbria, England) was a multitalented German artist. Schwitters´ life was marked by various health problems that never have been discussed in all their biographical and medical aspects according to contemporary medical knowledge. The fourteen-year-old Schwitters had his first seizure after a traumatic experience. When he was about 18 or 19, the seizures reached a climax, and he had several fits per day. Then they suddenly eased and became more and more infrequent, until, in the last 10 years of his life, he only had some five fits altogether. Today this seizure disorder could be classified as psychogenic non- epileptic seizures rather than true epilepsy as concluded in academic studies so far. This major impairment of his health in his adolescence evidently motivated Schwitters to become an artist.
Outlawed by the Nazi regime as a “degenerate artist”, he lived as a refugee in Norway and England from 1937 till his death, his career as an internationally recognized writer and artist destroyed. Above all, he developed complaints, symptoms and organ manifestations typical for untreated severe malignant hypertension, such as congestive heart failure, stroke, and visual disturbances. During his last two years of life in 1946-1947 he gathered his creative powers, painted, sculpted and wrote poetry in great creative euphoria.
In conclusion, the extensive written correspondence has made it possible to classify Schwitters’ illnesses according to contemporary medical knowledge, despite the fact that no medical documents were available.
Keywords: Kurt Schwitters; Merz Barn; Psychogenic non-epileptic seizures; Untreated malignant hypertension; Health and art.
Citation: Zeidler H, Webster G. Kurt Schwitters´ medical biography: Health problems and impact on creativity. J Clin Images Med Case Rep. 2023; 4(11): 2712.
Introduction
Kurt Schwitters (born June 20, 1887 in Hannover, † January 8, 1948 in Kendal, Cumbria, England) was a multitalented German artist (Figure 1) [1]. He now ranks among the most important artists connected with Dadaism, the interdisciplinary and culturally critical art movement that developed as a reaction to the First World War and combined primitive with modern techniques Schwitters himself avoided the term Dada, referring to his multimedia work as MERZ, a meaningless syllable he cut out of an advertisement for the Commerzbank. MERZ can be understood as Schwitters’ idiosyncratic response to Dada, an approach that involved the creation of new forms of collage and assemblage, often using refuse, found objects and discarded items. Schwitters’ MERZ output included a wide range of abstract artworks and also a series of ground-breaking sculptural environments. The first Merzbau (a name later given to all his room-filling constructions) took shape in Schwitters’ parents’ apartment in Hannover between 1923 and 1936; both the second Merzbau in Oslo and the third- the so-called Merz Barn in the English Lake District-were created in exile. Very little of these pioneering works has survived (see whole biography in: [2]).
Schwitters’ experimental MERZ writings include prose works, critical essays and phonetic and typographical poetry. He often employed fragments of language extracted from printed material or overheard conversations to create literature of an unexpected and often comical nature. Schwitters’ multifaceted work may have been essentially humorous, but his intentions were serious and his networking skills exceptional. His avant-garde MERZ magazine, published between 1923 and 1932, was in part multilingual; its issues included his own and others’ literary and visual works, an exhibition catalogue, a gramophone record, fairy tales, contributions on architecture and typography and a scripted 35-minute sonata in sound. Above all, in an increasingly polarised society, he investigated the border areas between established categories, challenging their frontiers and opening them up to adjustment and exchange.
Schwitters suffered from different health disorders throughout his life which to a large extent were described in a biography published in 1997 [3]. Below we provide a more comprehensive and more carefully documented overview and analysis of Schwitters’ known diseases, considering both their medical aspects and their overall impact on his creativity.
Seizure disorder
In autumn 1901, the fourteen-year-old Schwitters suffered a first seizure during a stay at the family’s summer house in rural Isernhagen, north of Hannover. In his own words: ‘I had a small garden there. Roses, strawberries, an artificial mountain, a constructed pond. In autumn 1901, village boys destroyed my garden before my eyes. The upset gave me St. Vitus’ Dance (in German Veitstanz). Sick two years, completely unable to work.’ [4].
We don’t know why Schwitters used the German term Veitstanz. St. Vitus’ Dance is an historical term for the spasmodic convulsions of a person suffering from the nervous disease chorea major (Huntington), a genetic neurodegenerative disease, and chorea minor (Sydenham chorea), one possible manifestation of rheumatic fever. Sydenham chorea usually manifests in school children and adolescents; it is triggered through a streptococcal infection and associated with arthritis and heart disease, manifestations not known from Schwitters’ biography. Moreover, recurrences of the chorea range only from one month to two years, but fits of convulsions plagued Schwitters for the next four decades, if with diminishing intensity [5].
In December 1947, the artist’s son Ernst described the symptoms of his father’s attacks as follows: ‘The fits last from 1/2 an hour to 3-5 hours. He usually is practically unconscious, shrieks and shouts just sounds and makes a dreadful snoring noise, while clinching his fists and “hammering” them on the ground or bed, or wherever he lies. The first “warning” of an approaching fit is generally unusual nervousness, quick-temper and varivarious movements with the head and the shoulders and arms.
Sometimes Daddy feels the fit coming on and tells you so himself. Then he usually lies down on a bed by himself. Sometimes he only complains about violent headache and pulls his head back time and again. The only thing to do, and the only cure, is to lie him down immediately and to give him a good dose of BALDRIAN (Authors’ note: Baldrian is the German name for Valerian, Valeriana officinalis, a herb native to Europe and parts of Asia. Valerian root has a long history of use as a sedative [6]) a quarter of a tumbler full, 50/50 with cold water. Only very seldom will this stop the fit before it comes through, but will ease him and help him to overcome the fit quicker. After a fit he is immediately completely “normal” again, but very tired, and usually sleeps for 12-16 hours afterwards’ [7].
When Schwitters was about 18-19 they reached a climax, during which he had several fits per day.
Then they suddenly eased and became more and more seldom; until, in the last 10 years, he only had some 5 fits altogether’ [7]. Although Schwitters’ attacks of convulsions became far less frequent after 1918 they could still be severe enough to land him in hospital, as reported by himself: ‘I thought about how I was carried to a hospital because of an epileptic seizure on the street in Dortmund.’ [8]. In 1940 he had one of his final attacks as a refugee from the Nazi regime in a British internment camp on the Isle of Man, probably triggered by the unbearable stress of his situation (information of one of the interviews of Gwendolen Webster with Ernst Schwitters, cited in [3]).
Quite apart from his seizure disorder, Schwitters was obsessed by his health. Wherever he went, he carried a supply of various remedies in a suitcase and as he never threw any medicine away, the stock accumulated to daunting proportions over the years (information from one of the interviews of Gwendolen Webster with Ernst Schwitters, cited in [3]). The only available doctor’s prescription is from 1926 and contains tablets of the drug Veramon (Authors’ note: personal information from Isabel Schulz, Kurt Schwitters Archive, Hannover). Veramon® was a barbital and amidopyrine combination drug from the Schering-Kahlbaum AG company with the indication as sleeping pills and sedatives [9]. It may be that Schwitters took Veramon® in Germany (at a time when his son would have been too young to remember) and that in exile he only had recourse to non-prescription remedies such as Valerian.
Overall, although no medical documents or electroencephalogram measurement are available, the reported features of his seizure attacks cannot be classified as true epileptic disease as noted in biographies so far. However, the description of a convulsive attack by Schwitters’ son Ernst fits best with the diagnosis of psychogenic non-epileptic seizures (PNES). PNES is a type of functional neurological disorder that semiologically may look like epileptic seizures, but is not due to an underlying epileptic activity; it is thought to be caused by a complex set of interrelated psychological, social, biological factors, and is often associated with psychological stressors [10]. Given the clinical similarity with epilepsy, misdiagnosis is common [11]. Typical symptoms of PNES are frequent situations triggering emotional conflict, long duration of the fits and vocalisation with crying or weeping. The effects are therefore very different from the rhythmic, generalized convulsion characteristic of epileptic convulsions (Table 1) [12-16]. Till now, a genetic disposition to seizures has been suspected, due to the reported epilepsy of the father of Schwitters’ mother [4]. Given the fact that PNES is frequently misdiagnosed as an epileptic disorder, this family history is also doubtful in view of true epilepsy.
People with PNES have depression, as reported in large studies, with a prevalence of 30% to 48% [17]. This comorbidity could also exist in Schwitters’ PNES disease on the basis of his autobiographical statement: ‘My basic trait was melancholy’ [4]. In addition, Helma, Schwitters’ wife, reminisced in a letter to him: ‘I know that at Ernst’s age (i.e., 22 years) you were just as miserable all your letters of the time breathe melancholy.’ [18]. Schwitters seems to have suffered from severe depression after he left the Dresden Academy, writing poems about death and undertaking long solitary hikes through Thüringen and Saxony. Presumably he suffered occasional bouts of severe depression, although few people were aware of this. Most subscribed to the view that ‘none of the four humours was more alien to his nature than melancholy’ [19]. His depression did not spring from doubts about the validity of his work; he was always convinced that future generations would come to recognise his importance as an artist, and time has borne him out [3]. His fits of depression may well have followed great bursts of energy that absorbed him so entirely, but the swings of mood in his private life are seldom documented, for he kept no diaries [3].
Health problems trigger Schwitters’ decision to make art his career
This major impairment of his health at the age of fourteen evidently motivated Schwitters to become an artist. In his own words: ‘My interests changed because of the illness. I discovered my love for art. Initially, I composed rhyming couplets in the manner of music-hall comedians. During a full moon one autumn night I noticed the clear, cold moon. From then on, I composed poetry in a lyrical sentimental manner. Then music seemed to me to be the art. I learned musical notation and played music all afternoon. In 1906, I saw my first moonlit landscape in Isernhagen and started to paint. One hundred water-colour landscapes by moonlight, painted from nature. Lit by stearin candles. I decided to become a painter. Usual parental opposition: first the Matura, then by all means. Attended art school in the evening and slowly became academic’ [4]. The traumatic experience of the destruction of the idealised form of nature which he had cultivated and the trigger thereby of his seizures has been interpreted from a psycho-biographical perspective as indicating that that all his creative activities emerged in a compulsive, repetitive manner: ‘In its capacity to create a whole from fragments, collage could represent Schwitters’ ever-present desire to unify the fragmented, to rebuild something that had been destroyed, and to control his shattered surroundings’ [20]. That may also be reflected in Schwitters’ own words written after the First World War: ‘Everything was broken anyway, and the task was to build something new from the broken pieces. But that’s Merz. It reflected the revolution in me, not as it was, but as it should have been’ [21]. These psychological defence mechanisms may also be translated to the creation of the Merzbau: ‘The idea that Schwitters could create something which would prove safe from the violence and repression of the outside world was a powerful one, allowing him to transform the anger, fear, pain and mourning he experienced into its antithesis: something he could create and control, both a sublimation and a defence’ [19]. Certainly from 1933 Schwitters’ seizures endangered him in view of the new ‘racial hygiene’ laws. The theory of the Merzbauten as refuge has, however, been contested, given that the Merzbauten in Hannover and Oslo were permanently under threat of destruction (the first by the Nazis and the second by the Norwegian police, who kept Schwitters under permanent observation); Schwitters literally worked himself to death on the third Merzbau, desperate to finish it in the full knowledge he had not long to live. In addition, the construction of all three Merzbauten required extremes of physical endurance at a time when the political situation meant that Schwitters was under intense pressure. However, the Merzbauten are interpreted, they cannot be ignored in an account of his medical history.
Health problems in later years and death
The first notification that Schwitters had chronically high blood pressure is documented in 1941 when he had immigrated to Britain. Over the next years he developed complaints, symptoms and organ manifestations typical for untreated severe hypertension (Table 2). Schwitters was not provided with antihypertensive therapy such as reported in a letter: ‘Normal would be for me 170. But Dr. Lancaster got it down now to 205, and Dr. Johnston says, to lower it more would render my circumstances be more dangerous than it is now. He says it goes up, because the heart has not enough movement’ [22]. It is noteworthy that this was standard medical practice at the time. In the 1946 edition of Tice’s Practice of Medicine (one of the leading textbooks of medicine at the time), Scott advised: ‘May not the elevation of systemic blood pressure be a natural response to guarantee a normal circulation to the heart, brain and kidneys (‘essential’ hypertension). Overzealous attempts to lower the pressure may do no good and often do harm. Many cases of essential hypertension not only do not need any treatment but are much better off without it’ [23]. It is therefore hardly surprising that Schwitters suffered common manifestations of untreated hypertension such as congestive heart failure, stroke, and visual disturbances (Table 2) [24,25].
weight loss and the rapid course of the disease may indicate a malignant or accelerated hypertension [26]. Malignant hypertension is defined by severe Blood Pressure (BP) elevation (commonly >200/120 mmHg) associated with advanced bilateral retinopathy (hemorrhages, cotton wool spots, papilledema) [27]. Schwitters’ BP values fulfil this definition and the eye symptoms (scotoma that rendered him unable to paint) are compatible with visual disturbances caused by severe hypertensive eye disease related to clinical signs of hypertensive retinopathy, hypertensive choroidopathy, and hypertensive optic neuropathy visualized today with modern retinal imaging techniques [28]. In addition, it can be speculated that the bleeding from the lungs and the bloody cough over several weeks (Table 2) could have been the manifestation of Diffuse Alveolar Haemorrhage (DAH), a rare complication from heart failure and/or malignant high blood pressure [29,30]. DAH induced by severe hypertension is commonly accompanied by renal dysfunction, fever, and progressive anaemia, comorbidities not reported in the case of Schwitters. Furthermore, mortality is 20% to 100%, which indicates that in Schwitters’ case an unusually benign, self-limiting form of DAH would have to be suspected. But without data from modern diagnostic techniques including chest radiography, contrast-enhanced multislice computed tomography with CT angiography, and bronchoscopy the correct diagnosis remains questionable. Potential differential diagnosis of massive haemoptysis or the bleeding from the lungs in the case of Schwitters would be primary idiopathic small vessel vasculitis, bronchiectasis, bronchitis, pneumonia, and neoplasia [30].
Table 1: Main clinical features to differentiate between sydenham chorea, epileptic seizure and psychogenic non-epileptic seizure [compiled from 12-16].
| Clinical features | Sydenham chorea | Epileptic seizure | Psychogenic non-epi- leptic seizure |
|---|---|---|---|
| Trigger | Streptococcal pharyngitis, caused by group Astreptococcus | Rarely | Frequent, e.g. conflict si- tuation |
| Duration | Mostly self-limiting, seldom chronic recur- rentforms | Usually no morethan 2-3 minutes | From > 3 minutesto hours |
| Type of involuntary movements | Classical chorea (= uncoordinated jerk-ing movements, whichmainly affect the face, hands, and feet), tics,ballistic movements |
Rhythmic, generali- zed | Alternating intensity, frequency and localization of movements, side-to-side head motions |
| Vocalization | Not a commonfeature | Very rare,at the be- ginningof the sei- zures | lctal crying orweeping. Present not only at the beginning of the event, can fluctuate, persist and be present,with different pitch intensities, throughout thewhole course of the lctal epi- sode |
Table 2: Schwitters’ complaints, symptoms, and organ manifestations related to chronic hypertension (compiled from [3]). Medical comments oriented on Braunwalds textbook of heart disease [24].
| Year | Manifestations | Medical comment |
|---|---|---|
| 1940 | duringemigration to Norway frequent trou- ble withhis eyes | Altered vision assign of hypertensive retinopa- thy |
| 1941 | “Bloodpressure is slightly better, 180to 130. I'm feeling fine, justa little short of breath.” + Struggling for breath. Bad attackof scotoma that he hadbeen unable to paintfor weeks. He wasdisplaying all the symptoms of chronic high blood pressure. |
Dyspnoea as asign of left ventriclehypertro- phy; alteredvision as sign of hypertensivereti- nopathy |
| 1944 | Temporary paralysis on one sideof his body | Stroke (hypertensiveencephalopathy?) |
| 1946 | “Bloodpressure 230, even higher than the time ofhis stroke (210). Heartbeat increases in speedwhen moving or slightly excited. Then he cannot seeanything for hours, but sees wonderful colorsthat are constantly moving.” ++ |
Palpitations asa signof left ventricle hypertro- phy; alteredvision as sign hypertensivereti- nopathy |
| 1947 | He lost weight, and hisblood pressure was still fartoo high. Desperate struggles for breath. Severe attack of asthma.Asthma at- tacks became morefrequent. “Hehad asthma, between 5 and6 hours,got digitalis.” +++ “Cardiac asthma has turned into Merzasthma and the resultis a very bad heart.” ++++ |
Cardiac asthmaas the medical condition of shortness of breath that is associatedwith un- derlying congestiveheart failure |
| July 1947 | Cough a streamof blood. Haemorrhage from the lungswhich lasted for ten hours. Three doctors cameto attend him and he wasgiven cocaine and morphine. For weekshe coughed up clots of blood. He could onlyget up for half anhour a day be- fore he was exhausted. |
Haemorrhage fromthe lungs and the bloodycough for several weeksmay have been a rare complication of heart failureand/or malignant hypertension [29, 30] |
| August/ September 1947 | He couldfeel his heart pounding at the slightest upset andhe was still losing weight. | Palpitations asa signof underlying congestive heart failure |
| November 1947 | He suddenly passedout and hit his headon a piece of stone on the floor | Fainting episode as sign ofcongestive heartfailure |
| December 1947 | He walkedto the Pierces' house, he suddenly collapsed.He struggled for air, tried to raisehimself and couldn’t. The doctorprescribed morphine and digitalis.His condition deterio- rated rapidlyand in the thirdweek in Decem- ber he was takento Kendal hospital. By Christmas he had contracted bronchitiswhich turned intopneumonia. He lay ina morphine delirium. | Fainting episode as sign ofcongestive heartfailure |
| January 1948 | He had beencomatose for manydays. He died on January 8th. | Death certificate: acute pulmonary oedemaand myocarditis |
+ see p.170 in [25]; ++ Correspondence Ernst Schwitters from Ambleside, December 1,1946. Sprengel Museum Hannover, Kurt Schwitters archive, Hannover, inventory number: que 06838814; +++ Correspondence Ernst Schwitters from Richmond, February 12, 1947. Sprengel Mu- seum Hannover, Kurt Schwitters archive, Hannover, inventory number: que 06838690; ++++ see p. 279 in [25].


Between July 1947 and November 1947 Schwitters’ health further worsened with increasing signs of heart failure, and in December he contracted bronchitis which turned into pneumonia (Table 2). Finally, he was comatose for many days and died on January 8th 1948. The doctor’s certificate gave the cause of death as acute pulmonary oedema and myocarditis, although it remains completely unclear how the diagnosis of myocarditis was made.
Interrelation between health and art
‘There were moments of depression, but nevertheless he had found the way he wanted to live, he had friends to support and encourage him in that existence and the benefit of that most precious asset, a partner able and willing to relieve him of the burdens of daily life so that he could devote himself totally to his work’ (Information given in [3]).
When the German National Socialists took power in 1933, Kurt Schwitters was defamed as a ‘degenerate’ artist. He was banned from selling his artworks, his writing was condemned as ‘bolshevist’ and he was deprived of his main income as a typographer. In 1937 Schwitters moved to Norway and never achieved more than refugee status for the remainder of his life. In the steeply sloping garden of his apartment in Lysaker, near Oslo, he erected (from scratch) a two-floor studio containing a new room sculpture, a second Merzbau (‘Merz building’) named Haus am Bakken. The suggestion came from his son Ernst, who hoped that it would drive away his father’s bouts of depression. Indeed, Schwitters wrote in October 1937: ‘I am building a new studio as a visible sign that a new life is beginning for me. It has to begin, I’m only fifty years old, one can begin again at that age. In all, life is so cruel that one shouldn’t have been born. With this premise one can live extremely well’ (Letter to K. Dreier, 13 October 1937, cited p. 284 in [3]).
Nevertheless, at other times depression overcame him. In the poem ‘Gefangen’ (‘Imprisoned’), he refers to himself as a dried leaf, a man lying in the valley of death, one who is punished because he has committed the crime of existing. ‘Haven’t I lost enough?’ (Cited p. 317 in [3]). An unfamiliar, rarely expressed, resignation showed itself in a letter of May 1946: ‘I have very high blood pressure, so that I would not survive a normal illness. Why should I, anyway?’ (Letter to E. Bergmann-Michel, 23 May 1946, cited p. 365 in [3]).
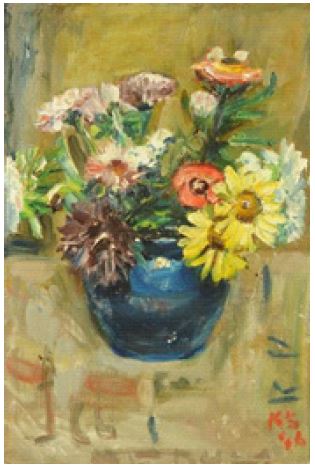
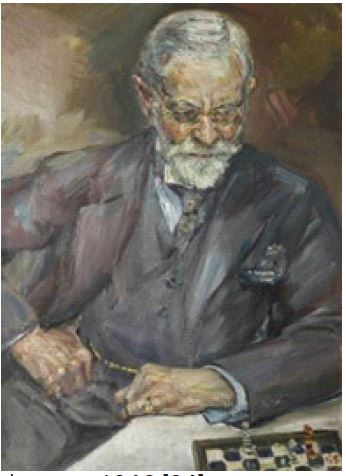
The last period of Schwitters’ life, in exile in the rural environment of Ambleside in the English Lake District, from 1945 until his death early in 1948, is marked by extensive creativity despite severe health problems. He diligently painted portraits, landscapes, and flower pieces. ‘One can tell from his best portraits that they are painted with head and heart, and not, as is sometimes disparagingly said, merely as commissions for a living although Schwitters daily income came solely from the income he earned from portrait commissions and the occasional sale of landscape paintings or still lifes’ [32]. ‘In the vibrancy of his paintings there is no sign that he was a sick man. This remarkable vitality, with which he approached the various plants in the most varied of ways, is even contained in his flower pieces’ [32]. (Figure 2) [33] Schwitters painted also Dr. George Ainslie Johnston, his faithful doctor and an amiable chess partner, in gratitude for saving his life (Figure 3) [34]. Sitting passively for hours was not something that came easily to the doctor. Kurt´s solution was to start a game of chess: ‘I don´t know whether to let him win - then he has a friendly expression, but people will think I´m a bad chess player - or shall I win, then his expression will be unfriendly and people will think I´m a bad painter.’ (Letter to C. Spengemann, 27 May 1946, cited p. 361-362 in [3]). A self-portrait painted in 1947 shows a serious, skeptical Schwitters who appeared relatively young despite his severely impaired health at the time (Figure 4) [35].
‘Schwitters incessantly explored the countryside and brought parts of it back to take their place in the collages and constructions he made: Pieces of bone, twigs, pebbles and shells, as well as the familiar papers and wrappings-but now even these were, of course, mainly English’ [36]. In the last year of his life, from January to December 1947, Schwitters created no less than 213 collages [37]. The mood of passing and of transience resonates in these collages from the English period [38]. Moreover, the amazing productivity may be psychologically interpreted as an expression of relief at having survived the war; or as an expression of the fear of losing creative power in the face of deteriorating health [37]. The sculptures of these years echo natural processes; smooth plaster forms, often coloured, canes blocked into cement, branches he had collected [36].
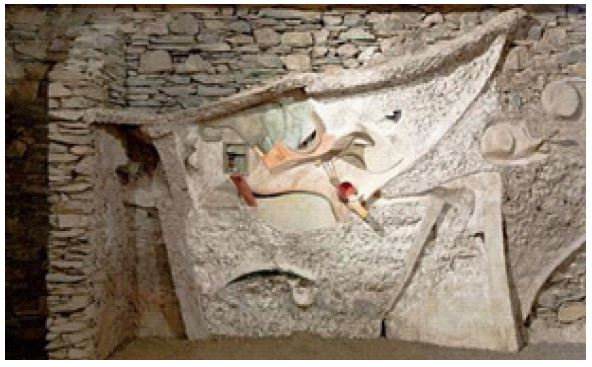
The chief work of this last work phase is the Merz Barn. In 1947, Schwitters started his final Merzbau on the estate of Harry Pierce, a landscape architect. It was housed in an unused straw barn in Elterwater, a few miles from Ambleside, and named the Merz Barn. Only a fragment, now known as the Merz Barn Wall, incomplete at his death early in 1948, has survived. In 1965 it was translocated and restored, and can now be seen on display in Newcastle University’s Hatton Gallery (Figure 6) [39]. The Merz Barn could be regarded as the freest, happiest, most organic of all his works, a replacement for the garden he lost at the age of 14, a creation connected to the environment, to nature, to the universe [40].
Conclusion
Understanding Schwitters’ art as a whole requires knowledge of his suffering and illnesses. His extensive written correspondence and few autobiographical writings have made it possible to classify his illnesses according to contemporary medical knowledge, although no medical documents were available. The medical history of Kurt Schwitters offers an instructive example of how a major health impairment triggered the decision to make art his career: in this case, it was a convulsive disease recognized today as psychogenic non-epileptic seizures provoked by a traumatic experience in adolescence. Of equal importance were the multiple health problems in later life that led to his death, which resulted from untreated severe malignant hypertension. The manner in which Schwitters coped with severe diseases during the last years of his life provides an informative example of how he continued to channel his debilities into creativity and into the production of exceptional artistic late work.
References
- Kurt Schwitters, before 1927, on a photograph by Genja Jonas. 2023.
- Kurt Schwitters. 1887-1948. 2023.
- Webster G. Kurt Merz Schwitters. A biographical study. Cardiff: University of Wales Press. 1997.
- Schwitters K. In Walden H (Ed.) Sturm-Bilderbuch IV. Berlin: Der Sturm. 1920.
- Aron A, Freeman J, Carter S. The natural history of Sydenham’s chorea. Review of the literature and long-term evaluation with emphasis on cardiac sequelae. Am J Med. 1965; 38: 83-95.
- WebMD. Valerian- Uses, Side Effects, and More. 2023.
- Schwitters E. Letter from Ernst Schwitters to Edith Thomas (‘Wanty’) about his father’s health and his wish to travel to the UK to see him. 2023.
- Schwitters K. Das literarische Werk. Band 2, Prosa 1918-30. Lach F (ed) Cologne: DuMont, 1973-1981
- Barbital https://de.wikipedia.org/wiki/Barbital. 2023.
- Asadi-Pooya AA, Brigo F, Tolchin B, Valente KD. Functional seizures are no less important than epilepsy. Epilepsy Behav Rep. 2021; 16: 100495.
- Gorenflo R, Ho R, Carrazana E, Mitchell C, Viereck J, Liow KK, et al. Identification of risk factors and distinguishing psychogenic nonepileptic seizures from epilepsy: A retrospective case-control study. Clin Neurol Neurosurg. 2022; 217: 107221.
- Walker KG, de Vries PJ, Stein DJ, Wilmshurst JM. Sydenham Chorea and PANDAS in South Africa: Review of Evidence and Recommendations for Management in Resource-Poor Countries. J Child Neurol. 2015; 30:850-859.
- de Teixeira AL, Cardoso F, Maia DP, Sacramento DR, Mota Cde C, Meira ZM, et al. Frequency and significance of vocalizations in Sydenham’s chorea. Parkinsonism Relat Disord. 2009; 15: 62-63.
- Leibetseder A, Eisermann M, LaFrance WC Jr, Nobili L, von Oertzen TJ., et al. How to distinguish seizures from non-epileptic manifestations. Epileptic Disord. 2020; 22: 716-738.
- Anzellotti F, Dono F, Evangelista G, Di Pietro M, Carrarini C, Russo M, et al. Psychogenic Non-epileptic Seizures and Pseudo-Refractory Epilepsy, a Management Challenge. Front Neurol. 2020;11:461.
- Baslet G, Bajestan SN, Aybek S, Modirrousta M, D Clin Psy JP, Cavanna A, et al. Evidence- Based Practice for the Clinical Assessment of Psychogenic Nonepileptic Seizures: A Report from the American Neuropsychiatric Association Committee on Research. J Neuropsychiatry Clin Neurosci. 2021; 33: 27-42.
- Patron VG, Rustomji Y, Yip C, Jenkins LM. Psychiatric Comorbidities in Functional Neurologic Symptom Disorder. Pract Neurol (Fort Wash Pa). 2022; 21: 71-75.
- Letter from Helma to Kurt Schwitters, February 15, 1940. Sprengel Museum Hannover, Kurt Schwitters archive, Hannover, inventory number: que 06838920
- Hans Freudenthal in Kurt Schwitters Almanach 9. Erlhoff M, Stadtmüller K (eds) Hannover: Postskriptum Verlag, 1990, p. 16
- O’Dowd Clare. Kurt Schwitters’s Merzbau: Chaos, Compulsion and Creativity. Moveable Type 2009; 5.
- Schmalenbach W. Kurt Schwitters. München, Prestel. 1984; 32.
- Correspondence to Ernst Schwitters, dated Ambleside, 1 January 1946. Sprengel Museum Hannover, Kurt Schwitters Archive, Hannover, inventory number: que 06838814.
- Kotchen TA. Historical trends and milestones in hypertension research: a model of the process of translational research. Hypertension. 2011; 58: 522-538.
- Braunwald E, Zipes DP, Libby P. Heart Disease. A Textbook of Cardiovascular Medicine. 6th Edition. Philadephia: Saunders. 2001.
- Schwitters K. Wir spielen, bis uns der Tod abholt. Briefe aus fünf Jahrzenten. Nündel E (ed) Frankfurt/M-Berlin: Ullstein. 1986.
- Vaziri ND. Malignant or accelerated hypertension. West J Med. 1984; 140: 575-582.
- Unger T, Borghi C, Charchar F, Khan NA, Poulter NR, et al. International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension. 2020; 75: 1334-1357.
- Konstantinidis L, Guex-Crosier Y. Hypertension and the eye. Curr Opin Ophthalmol. 2016; 27: 514-521.
- Saha BK, Chong WH. Diffuse Alveolar Hemorrhage in Cardiac Diseases. Lung. 2021; 199: 103-112.
- Hamaguchi S, Suzuki H, Hamaguchi M, Iwasaki M, Fukuda H, et al. A rare case of alveolar hemorrhage with hypertensive emergency. Medicine (Baltimore). 2022; 101: e30416.
- Lordan JL, Gascoigne A, Corris PA. The pulmonary physician in critical care. Illustrative case 7: Assessment and management of massive haemoptysis. Thorax. 2003; 58: 814-819.
- Burkett ME. Das fi gurative Werk von Kurt Schwitters. In: Erlhoff M, Stadtmüller K (eds) Kurt Schwitters Almanach No 8. Hannover: Postskriptum Verlag. 1989; 57-66.
- Mitchells Antiques & Fine Art, antiques & fine art sale. 2015; 1002. https://www.mitchellsauction.co.uk/antiques-fine-art/forthcoming-sales-events/archive/0533/?search=true&lot=&keyword=kurt+schwitters&cat
- The Armitt Museum and Library. https://artuk.org/discover/artworks/ search/keyword:schwitters-referrer: global-search/page/2. 2023.
- Kurt Schwitters, self-portrait, 1947. https://goteborgskonstmuseum.se/en/the-collection/hjalmar-gabrielsons-portrait-collection/. 2023.
- Elderfield J. The last work of Kurt Schwitters. Artforum 1969 https://www.artforum.com/print/196908/the-last-work-of-kurt-schwitters-36473. 2023.
- Cardinal R, Webster G. Kurt Schwitters. German Edition. Ostfildern: Hatje Cantz. 2011.
- Büchner J. Zeugen der Vergänglichkeit. In: Sprengel Museum Hannover (2 nd. edition). Kurt Schwitters. 1887-1948. Dem Erfinder von MERZ zu Ehren und zur Erinnerung, zur Retrospektive 1986, zum 100. Geburtstag 1987. Berlin: Propyläen. 1987; 212.
- From there to here-the fascinating journey of the Merz Barn Wall. 2023.
- Nündel E, Kurt Schwitters. In Selbstzeugnissen und Bilddokumenten. Reinbek bei Hamburg: Rowohlt. 1981; 125.