
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Unusual presentation of antepartum lumbosacral plexopathy: A rehabilitation approach
Anindya Debnath*; Jaya Das
Physical Medicine and Rehabilitation, St. John’s National Institute of Medical Sciences, Bangalore, India.
*Corresponding Author : Anindya Debnath
Physical Medicine and Rehabilitation, St. John’s National Institute of Medical Sciences, Bangalore, India.
Email: anindyadebnath@gmail.com
Received : Oct 30, 2023
Accepted : Nov 23, 2023
Published : Nov 30, 2023
Archived : www.jcimcr.org
Copyright : © Debnath A (2023).
Abstract
Background: This case report focuses on a woman in her late thirties (gravida three para three) referred from Neurology to Physical Medicine & Rehabilitation department due to pain, lower limb weakness, walking difficulties, and dependence in daily activities. Her symptoms, which began during the second trimester of pregnancy, progressed from burning sensations in her feet to muscle weakness affecting her legs and thighs in the peripartum period.
Case presentation: Following delivery, diagnostic investigations indicated lower creatine phosphokinase levels, MRI findings showed muscle atrophy in the posterior compartment of both thighs, and an electromyography and nerve conduction study confirmed bilateral lumbosacral plexopathy.
Treatment and outcomes: Rehabilitation commenced six weeks postpartum, but the patient faced challenges due to her functional limitations. The treatment included a multifaceted approach encompassing medical management, physical therapy, and occupational therapy. Notably, the patient demonstrated significant improvement within two weeks of inpatient rehabilitation.
Conclusion: This case underscores the effective management of antepartum lumbosacral plexopathy using a comprehensive rehabilitation strategy. Early intervention and a multidisciplinary approach are pivotal in achieving positive outcomes in similar clinical presentations.
Keywords: Ante natal; Rehabilitation; Pregnancy; Antepartum plexopathy; Lumbosacral plexopathy.
Citation: Debnath A, Das J. Unusual presentation of antepartum lumbosacral plexopathy: A rehabilitation approach. J Clin Images Med Case Rep. 2023; 4(11): 2715.
Introduction
A multimodal approach and teamwork are indispensable to deliver optimal care for our patients. This report recounts the management of a woman who presented with a rare case of pregnancy-induced bilateral muscle atrophy in the thighs due to lumbosacral plexopathy, necessitating a progressive rehabilitation strategy.
Lumbosacral plexopathy during pregnancy is an infrequent condition, typically associated with a favourable outcome. It often initiates with groin pain, followed by the onset of muscle weakness, primarily affecting the quadriceps and iliopsoas muscles, often accompanied by muscle atrophy. Sensory loss is less common. Electromyography (EMG) typically reveals denervation activity in muscles controlled by the upper part of the plexus, without paravertebral denervation activity [1].
The precise cause remains unknown. While postpartum femoral neuropathies and obturator nerve damage due to compression have been reported, the timing of symptoms in this case suggests possible involvement of foetal pressure on the plexus in the aetiology [2,3]. Recovery may take several months, but the prognosis is generally favourable. Patients should undergo rehabilitation to manage disability during the critical antepartum and postpartum periods [4].
Case presentation
A woman in her late thirties, who had given birth to a healthy baby girl via caesarean section six weeks ago, was referred to the Neurology department due to complaints of pain and weakness in both lower limbs. She had a history of hyperemesis gravidarum in all her previous pregnancies and had delivered all her children via caesarean section. Examination revealed reduced muscle mass in both thighs, and further investigations indicated muscular atrophy in the posterior compartments of both thighs along with signs of lumbosacral plexopathy.
Upon admission to the Physical Medicine & Rehabilitation department, her functional abilities were assessed. She could independently transition from a supine to a sitting position but was completely dependent for sitting to standing, standing, and walking. Regarding Activities of Daily Living (ADL), she could independently manage feeding, grooming, and dressing but required moderate assistance for toileting. Her static and dynamic sitting balance were good, but her standing balance was poor.
During a motor examination, she exhibited 4/5 strength in both hip flexors, 2/5 strength in both hip extensors, 3/5 strength in both hip abductors and adductors, 3/5 strength in both knee flexors and extensors, and 4/5 strength in both ankle dorsiflexors and plantar flexors. The straight leg test produced positive results bilaterally. Sensory examination revealed impaired light touch and pinprick sensation L3 to S2 and left L4 to S2 dermatomes. Knee and ankle reflexes were diminished bilaterally. On per-rectal examination, her anal tone was normal, and deep anal pressure, voluntary anal contraction, Ano Cutaneous Reflex (ACR), and Bulbocavernosus Reflex (BCR) were intact. She exhibited continence for both bowel and bladder functions, and the rest of her examination yielded unremarkable findings.
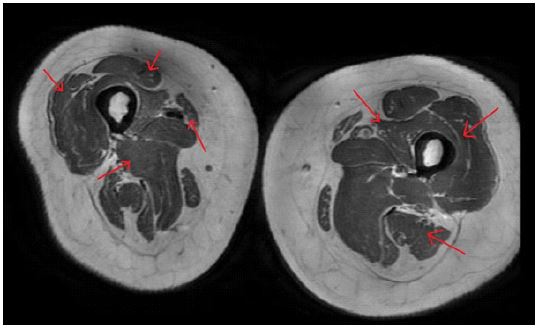
The patient’s blood investigations indicated normal CPK levels (22 U/L), plasma Vitamin D levels (27 ng/ml), and Vitamin B12 levels (438 pmol/L). Electromyography (EMG) revealed denervation of proximal hip and thigh muscles and nerve conduction studies (NCS) showed absent Compound Muscle Action Potential (CMAPs) in the left common peroneal nerve, severe reduction in the right peroneal nerve, and mild reduction in the right tibial nerve, along with the absence of F waves in bilateral common peroneal nerves; absence of sural Sensory Nerve Action Potential (SNAPs) bilaterally. MRI of the lumbosacral spine displayed a loss of lumbar lordosis, facet arthropathy at the L4-L5 and L5-S1 levels, and no evidence of demyelination (Figure 1). Additionally, MRI of both thighs indicated reduction in bulk of all muscles of both thighs with asymmetric predominance of posterior compartment muscles-compatible with myopathy without any features of myositis (Figures 2,3). These comprehensive findings played a crucial role in assessing the patient’s condition and guiding further management.
The patient’s comprehensive rehabilitation regimen encompassed both pharmacological and non-pharmacological approaches. In terms of pharmacological management, the patient was prescribed a combination of topical and oral analgesics, muscle relaxants, multivitamins, and Vitamin D supplements to effectively address her symptomatic needs.

Non-pharmacological interventions played a pivotal role in her rehabilitation journey. These interventions included graded strengthening exercises targeting the back and hip girdle muscles, such as bridges and straight leg raises, with a protocol of 2 sets of 10-12 repetitions which was gradually increased. Active assisted range of motion exercises, bedside hamstring and quadriceps stretching exercises were performed, amounting to a cumulative six hours daily.
Furthermore, the patient engaged in two hours of prone lying, and employed two-kilogram ankle weights on both sides to enhance specific muscle groups.
The occupational therapy component of the rehabilitation program was focused on transfers and balance training, Activities of Daily Living (ADL), and functional activity retraining to restore independence and quality of life. Additionally, physical therapy incorporated stretching and strengthening exercises tailored to target the gluteal, hamstring, and quadriceps muscles. The patient also underwent aerobic training and program to enhance her standing ability with knee support and gradually transitioned to gait training with the assistance of a walker and standing without assistance (Figures 4,5).


These synergistic therapies were designed to optimize the patient’s recovery and functional abilities. Architectural modifications were thoughtfully implemented to enhance safety and prevent falls, including the installation of grab handles and anti-skid mats.
Upon admission, the patient’s Functional Independence Measure (FIM) scored 58 out of 126, her Barthel index was 60 out of 100, she reported a Visual Analogue Scale (VAS) pain rating of 8 out of 10, and her Lower Extremity Functional Scale (LEFS) was 17 out of 80. However, at the time of her discharge, significant improvements were observed, with FIM at 119 out of 126, Barthel index at 85 out of 100, VAS pain rating reduced to 2 out of 10, and LEFS reaching 72 out of 80 (Table 1).
Table 1: The course of endoscopic treatments.
| Functional scales | Admission | Discharge |
|---|---|---|
| Functional Independence Measure (FIM) | 58 | 119 |
| Barthel Index | 60 | 85 |
| Visual Analog Score (VAS) | 8/1 | 2/10 |
| Lower Extremity Functional Scale (LEFS) | 17 | 72 |
The patient attended outpatient follow-up appointments at 3 and 8 weeks after her discharge. During these visits, she demonstrated complete independence in her daily activities and exhibited the ability to walk independently, with only minor lingering neurological deficits.
Discussion
The precise origin of this condition remains unknown. Postpartum compression neuropathies, such as femoral neuropathies after delivery and obturator nerve damage, have been documented as potential contributing factors. The onset of symptoms in this specific case suggests that pressure exerted on the plexus by foetal parts may have contributed to its aetiology. In a similar case series by Delareua et al. three cases of antenatal lumbosacral plexopathy (LSP) were discussed, all of which presented symptoms in the third trimester of pregnancy with no prior neurological issues. Two of these cases occurred during their first pregnancy. Thorough neurological examinations were conducted, X-ray spine results were normal, MRI ruled out myelopathy, and EMG revealed denervation in proximal hip and thigh muscles. Following physical therapy, all patients achieved complete recovery within 3-6 months post-pregnancy [1]. However, a comprehensive understanding of the exact causative factors of this condition is yet to be determined. Although recovery may extend over several months, the injury is typically self-limiting, and patients can anticipate a favourable outcome. Nonetheless, a rehabilitation program is essential to effectively manage their temporary disabilities.
Conclusion
This case highlights the uncommon occurrence of lumbosacral plexopathy, emphasizing the need for vigilance regarding neurological complications during pregnancy. When such complications arise, a thorough evaluation, including a detailed medical history, comprehensive physical examination, and relevant diagnostic tests, becomes imperative to guide proper management. Regardless of the rarity of the presentation, a multimodal approach is crucial for effective care, underlining the significance of timely diagnosis and rehabilitation in both typical and unusual cases. In this evolving landscape, rehabilitation plays an ever-expanding role in addressing emerging trends and concepts associated with these atypical neurological presentations, reinforcing the importance of a holistic approach to patient care.
Human subjects: Consent was obtained by participant in this study.
References
- Delarue MW, Vles JS, Hasaart TH. Lumbosacral plexopathy in the third trimester of pregnancy: A report of three cases. Eur J Obstet Gynecol Reprod Biol. 1994; 53: 67-8.
- Massey EW, Cefalo RC. Neuropathies of pregnancy. Obstet Gynecol Surv. 1979; 34: 489-92.
- Montag TW, Mead PB. Postpartum femoral neuropathy. J Reprod Med. 1981; 26: 563-6.
- Vargo MM, Robinson LR, Nicholas JJ, Rulin MC. Postpartum femoral neuropathy: relic of an earlier era? Arch Phys Med Rehabil. 1990; 71: 591-6.