
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
A case of metastatic lung tumor originating from pancreatic cancer detected by low-dose computed tomography lung cancer screening eight years after surgery
Hiroyuki Miura1*; Jun Miura2; Shinichi Goto3; Tomoko Yamamoto4
1Department of Thoracic Surgery, Akiru Municipal Medical Centre, Tokyo, Japan.
2Department of Surgery, Kyorin University School of Medicine, Tokyo, Japan.
3Department of Respirology, Akiru Municipal Medical Centre, Tokyo, Japan.
4Department of Pathology, Tokyo Women’s Medical University, Tokyo, Japan.
*Corresponding Author : Hiroyuki Miura
Department of Thoracic Surgery, 78-1 Hikida, Akiruno City, Tokyo 197-0834, Japan.
Tel: +81-42-558-0321;
Email: arowana@akiru-med.jp
Received : Oct 23, 2023
Accepted : Nov 24, 2023
Published : Dec 01, 2023
Archived : www.jcimcr.org
Copyright : © Miura H (2023).
Abstract
Although the prognosis of pancreatic cancer is poor [1], it could be expected by removing single lung metastases. We report a case of a lung cancer patient screened with Low-Dose Computed Tomography (LDCT) after 8 years of stage III pancreatic cancer. Considering this, it is rare to detect lung metastases after 8 years of pancreatic cancer surgeries.
Patients who have already completed their observation period should rely on screening to detect cancers of any organ. LDCT lung cancer screening aims to identify early-stage lung cancers. In addition, it also helps in the detection of metastatic lung tumors that cannot be noticed by simple chest X-rays in cancer patients whose observation periods have already ended.
Keywords: Low-dose CT; Metastatic lung tumor; Pancreatic cancer.
Citation: Miura H, Miura J, Goto S, Yamamoto T. A case of metastatic lung tumor originating from pancreatic cancer detected by low-dose Computed Tomography lung cancer screening eight years after surgery. J Clin Images Med Case Rep. 2023; 4(12): 2717.
Introduction
Studies showed that a 5-year survival rate for pancreatic cancer is only about 5%. However, the number of long-term survival cases has increased with the progress of chemotherapy [1]. Nevertheless, some cases of recurrence occur after a long time from surgery.
Low-Dose Computed Tomography (LDCT) lung cancer screening has shown to be useful in large-scale clinical studies in the United States [2] and Europe [3]. Likewise, in Japan, early detection of lung cancer in non/light smokers by LDCT screening led by the Japan Agency for Medical Research and Development is under way [4]. In this study, we report a lung metastasis, which originated after stage III pancreatic cancer after 8 years from surgery, and was detected by LDCT lung cancer screening.
Case report
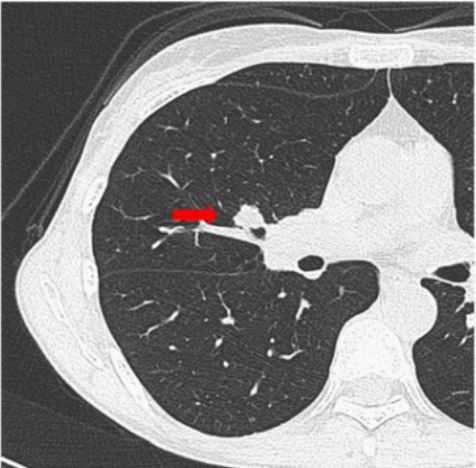
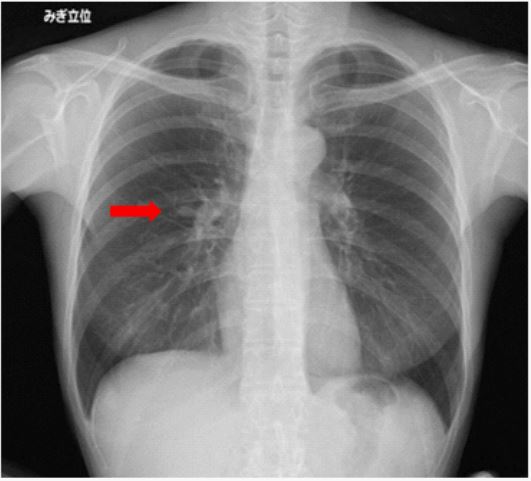
A 52-year-old woman presented with an abnormal shadow on LDCT lung cancer screening. Her family history was unremarkable with cancers, and she never smoked. Her chest CT scan revealed a 12 mm solid nodule in her right middle lobe (Figure 1A), whereas, her chest X-ray showed a small nodule in the right middle lung field mimicking a branch of pulmonary artery (Figure 1B). Blood tests showed a slightly elevated carcinoembryonic antigen at 5.9 ng/ml (normal 0-2.5 ng/mL), combined with hepatic dysfunction linked to high levels of aspartate aminotransferase at 57U/L (normal 8-33U/L) and alanine aminotransferase at 47 U/L (normal 4-36U/L). However, hemogram, renal function, carbohydrate antigen 19-9 (CA 19-9), Cyfla and pro-gastrin-releasing peptide (proGRP) were within normal ranges.
The patient was already diagnosed with pancreatic cancer at the age of 44 and underwent subtotal stomach-preserving pancreaticoduodenectomy after pre-operative radiochemotherapy with gemcitabine and tegafur. Her pathologic stage was III (pT3N1M0). She lived without recurrence for 5 years after her first operation and her observation periods ended.
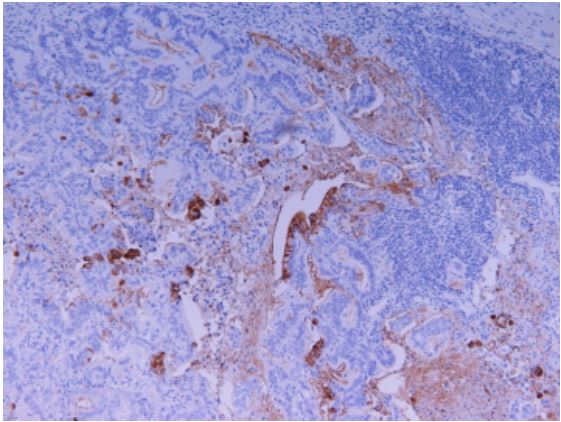
Her right middle lobe resection was done with a definitive diagnosis and an intra-operative confirmation of adenocarcinoma where a mediastinal lymph node dissection was added in accordance with lung cancer. Pathologically, the tumour size was 13×13×12 mm with a positive Cytokeratin 7 (CK 7), partially positive Thyroid Transcription Factor 1 (TTF-1) and CA 19-9 (Figure 2), negative CK20 and napsin A. The stainability was noted to be similar the primary pancreatic cancer. Therefore, the tumour was diagnosed as metastatic lung tumour originating from the pancreatic cancer. Metastasis was found only in the lymph node near the lung tumour.
Discussion
Less than 20% of pancreatic cancers are surgically resectable. Even though few patients can undergo surgeries, over 80% of patients relapse afterward. Even with macroscopic complete tumour resection and adjuvant therapies, the 5-year survival rate is only 20% [1]. However, if metastasis occurs only in the lung after pancreatic cancer treatment, a good prognosis can be expected. Sakaguchi et al. reported a review of literature about surgical treatment of metastatic pancreatic ductal adenocarcinoma and pointed out that overall survival after initial treatment varied from 51.0 to 85.9 months in metachronous lung metastasis [5]. Therefore, the removal of metastatic lung tumour originating from pancreatic cancer could be one treatment strategy.
Two randomised control studies have shown the usefulness of LDlow-dose CT screening, namely, the National Lung Screening Trial (NLST) in the United States [2] and the Dutch-Belgian lung cancer screening trial (NELSON) in Europe [3]. Eligible participants of NLST had either a history of cigarette smoking of >30 pack-years or were former smokers from ≤15 years ago. The relative reduction in mortality from lung cancer with LDCT screening was found to be 20%, and the rate of death was reduced in the LDCT group compared with the radiography group by 6.7%. On the other hand, the participants of NELSON trial were either current smokers with >15 cigarettes/day for >25 years or >10 cigarettes/day for >30 years or former smokers from ≤10 years ago. The cumulative rate ratio for death from lung cancer at 10 years was 0.76 in the screening group compared with the control group. Since both studies targeted heavy smokers, they are not considered for early detection of lung cancer for non-smokers or light smokers. The question arises about the effectiveness of LDCT for other than heavy smokers. In Japan, the Japanese randomized trial for evaluating the efficacy of low-dose thoracic CT screening for lung cancer (JECS Study) was currently on going. That was conducted to evaluate the efficacy of thoracic LDCT screening for lung cancer in non-smokers and smokers of <30 pack-years, in order to compare the rate of lung cancer deaths between LDCT screening and simple chest X-ray screening for non/light smokers [4]; The metastatic tumour of this patient was detected as a part of this screening programme.
Conclusion
LDCT can be a useful technique not only for early detection of lung cancer but also for early detection of metastatic lung tumor in cancer patients who have completed the observation period.
Declarations
Conflict of interest statement: The authors have no conflict of interest to declare.
Author contribution statement: The role of Dr Hiroyuki Miura and Dr Shinichi Goto is the conception and design of the work and the acquisition and analysis or interpretation of data for the work. Dr Jun Miura drafted the work and revised it critically for important intellectual content. Dr. Yamamoto diagnosed this cancer pathologically. All authors contributed to the final version of this manuscript and approved it to be published.
Ethics statement: Appropriate written informed consent was obtained for publication of this case report and accompanying images.
References
- Kleeff J, Korc M, Apte M, La Vecchia C, Johnson CD, et al. Pancreatic cancer. Nat. Rev. Dis. Primers. 2016; 2: 1-22.
- National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011; 365: 395-409.
- De Koning HJ, van der Aalst CM, de Jong PA, Scholten ET, Nackaerts K, et al. Reduced lung-cancer mortality with volume CT screening in a randomized trial. N. Engl. J. Med. 2020; 382: 503- 513.
- Sagawa M, Nakayama T, Tanaka M, Sakuma T, Sobue T. JECS study group. A randomized controlled trial on the efficacy of thoracic CT screening for lung cancer in non-smokers and smokers of <30 pack-years aged 50-64 years (JECS Study): Research Design. JJCO. 2012; 42: 1219-1221.
- Sakaguchi S, Valente R, Tanaka K, Satoi S, Chiaro MD. Surgical treatment of metastatic pancreatic ductal adenocarcinoma: A review of current literature. Pancreatology. 2019; 19: 672-680.