
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Treatment and rethinking: A case of well differentiated liposarcoma of spermatic cord
Wenjun MA; Qiang Long; Baoming Ren*
Department of Urology, XI’an No.3 Hospital, the Affiliated Hospital of Northwest University, Xi’an, Shanxi 710018, PR China.
*Corresponding Author : Baoming Ren
Department of Urology, XI’an No.3 Hospital, the
Affiliated Hospital of Northwest University, Xi’an,
Shanxi 710018, P.R. China.
Email: mwj_98@126.com
Received : Oct 31, 2023
Accepted : Nov 28, 2023
Published : Dec 05, 2023
Archived : www.jcimcr.org
Copyright : © Ren B (2023).
Abstract
Spermatic cord liposarcoma is very rare and characterized by a painless inguinal or scrotal mass. This is a case report of a 49-year-old man presenting with a mass in his left Inguinal, and the histopathological examination revealed a liposarcoma of the spermatic cord.
Citation: Wenjun MA, Long Q, Ren B. Treatment and rethinking: A case of well differentiated liposarcoma of spermatic cord. J Clin Images Med Case Rep. 2023; 4(12): 2722.
Introduction
Liposarcoma of the spermatic cord is a rare malignant disease, which may present like an inguinal hernia. The incidence of malignant spermatic cord tumors is 0.3 cases per million, and of those, the most common type is liposarcoma. Although they make up a minority of liposarcomas, dedifferentiated subtype is most concerning for aggressive behavior and rapid recurrence. They present typically from the fifth to seventh decades of life, as either an inguinal hernia or paratesticular mass as they descend into the scrotum. Given the rarity of this condition, most published data regarding management consists of case reports. From an academic medical system, we present a man in his late forties with an inguinal hernia and protracted five-year history of mild right lower quadrant pain. Consistent with published literature, his surgical management included radical orchiectomy with wide margins.
Case presentation
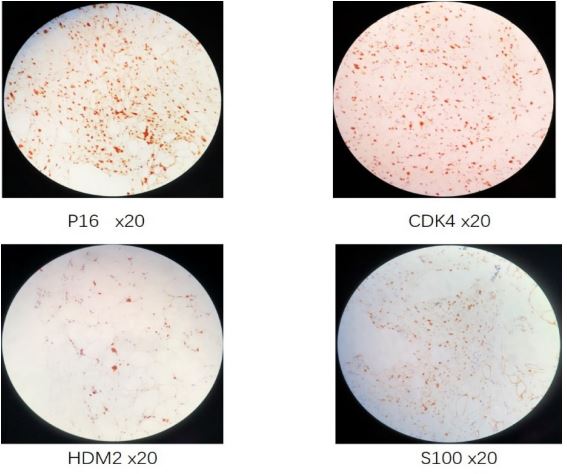
A 49-year-old gentleman presented complaining of left inguinal mass. There is no special history besides hypertension in the past. Special physical examination: The left groin can touch an obvious 10x6 cm mass, which is hard without tenderness, protrudes into the scrotum and has a clear boundary with the testis and epididymis. No obvious abnormality was found in blood routine examination, urine routine examination, liver and kidney function, human chorionic gonadotropin, lactate dehydrogenase and alpha fetoprotein. Ultrasound findings: isoechoic mass in the left inguinal area, with regular shape and uniform echo, considering the possibility of inguinal hernia. Preoperative misdiagnosis was left inguinal hernia. During the operation, it was found that a mass of about 10x6 cm in size could be seen in the left inguinal region, with smooth surface, adhesion with spermatic cord, clear boundary with testis and epididymis, and the tumor was completely removed during the operation (Figure 1). Postoperative pathological results: invasive well differentiated liposarcoma. Immunohistochemical results: MDM2 (+), CDK4 (+), p16 (+), S100 (+) (Figure 2). One month later, the patient underwent high ligation of spermatic cord and radical orchiectomy. Pathological report again after operation: no tumor tissue was found in testis, epididymis and lymph nodes, and tumor tissue was found in spermatic cord. The final modified diagnosis: well differentiated liposarcoma of the left spermatic cord. There was no tumor metastasis or recurrence after follow-up for more than 5 years.

Discussion
According to the WHO classification standards for soft tissue and bone tumors, liposarcomas can be divided into four main subtypes: Atypical lipomatoid tumors/well differentiated liposarcomas, Dedifferentiated liposarcomas, Myxoid liposarcomas and Polymorphic liposarcomas [1]. Liposarcoma usually occurs in the extremities and retroperitoneum, but rarely occurs in the testis. It has been reported in other cases that paratesticular liposarcomas are mostly appeared asymptomatic solid masses, which can be touched by physical examination. More than 90% of them originate from the spermatic cord. Most of them can be clearly distinguished from the testis, while epididymis and testicular capsule liposarcomas have unclear boundaries with the testis [2]. Since the first report of spermatic cord liposarcoma in 1845, only more than 200 cases have been reported internationally [3]. However, due to the relatively rare reports, it is easy to be misdiagnosed as inguinal hernia. In our report, the patient was misdiagnosed as inguinal hernia before operation because the painless inguinal mass protruded into the scrotum and the ultrasound suggested that the hernia was possible. However adequate physical examination by specialists and imaging examination before operation are helpful to differentiate diagnosis. For liposarcoma of spermatic cord, ultrasonography usually shows solid, hyperechoic and heterogeneous lesions; On CT, the most common manifestations were: round, well-defined, lowdensity adipose tissue with uneven density. Some tumor lesions were seen as bands or lobulated. On enhanced scan, some tumor parenchyma showed mild to moderate uneven enhancement; MRI can be used to assess the extent of tumor expansion. T1WI and T2WI are mainly high signal, with uneven distribution of internal signals, low or equal signal band like divisions or small nodules can be seen, and lipid compression sequence signals are mostly reduced [4,5]. Therefore, when ultrasound is not clear or the results are controversial, we suggest further pelvic CT or MRI examination, which can provide valuable advice.
The diagnosis of spermatic cord liposarcoma depends on the pathology. Immunohistochemistry and molecular detection of MDM2 and CDK4 are helpful for accurate diagnosis [1]. The strong immune reaction of liposarcoma to CDK4 and MDM2 can be used to distinguish liposarcoma from benign lipoma. In liposarcomas, the most specific immunohistochemical marker is S100 protein, which is expressed in 90% of liposarcomas [6]. The expression of p16 gene can be used to support the diagnosis of well differentiated liposarcoma and dedifferentiated liposarcoma. The pathological results of this patient showed that there were fibrous fat lobules with intact capsule, fat cells of different sizes, and large polymorphonuclear cells scattered in the tumor. The surgical margins were negative. Immunohistochemical results showed that: MDM2 (+), CDK4 (+), p16 (+), S100 (+), Vimentin (+), CD34/p53 (+, partial cells), Ki67 (+, 8%). The results were consistent with the diagnosis of well differentiated liposarcoma
For the treatment of spermatic cord liposarcoma, extensive local tumor resection+ radical orchiectomy is the main method [7]. In our case report, this patient was misdiagnosed as inguinal hernia before operation, so only complete resection of the tumor was performed during the operation. After pathological diagnosis, radical orchiectomy and local extensive resection were performed again. However, there is no consensus on whether patients with liposarcoma need further lymph node dissection, radiotherapy/chemotherapy or not. Reviewing previous literature, most researchers pointed out that adjuvant radiotherapy is usually not required except for cases with positive margin or local recurrence and poor prognostic factors. This patient was followed up for 3 years, and no local or distant metastasis/recurrence was found. Therefore, we suggest that only performe extensive resection for patients without distant metastasis, but adjuvant treatment for metastatic tumor/cases with postoperative recurrence or incomplete resection.
To sum up, spermatic cord liposarcoma is an extremely rare tumor. Its main clinical manifestations include irregular tumors of different sizes and medium soft texture in scrotum, spermatic cord or groin. Laboratory biochemical tests are mostly negative, and imaging examination show uneven solid lesions. The possibility of spermatic cord liposarcoma should be considered when fat bearing inguinal scrotal masses are seen. Surgical resection is the main treatment for spermatic cord liposarcoma. Regular reexamination should be carried out after surgery to find tumor recurrence early, and early treatment after recurrence is the key to ensure a good prognosis.
Conclusion
Liposarcomas are a very rare entity. The diagnosis before operation is difficult, and the treatment should be completely surgical excision. However, If the margin status is doubtful, a second look and excision is mandatory. Distant disease has not been reported, but local relapse is common and may occur even several years after primary therapy. A long follow-up period is necessary.
Declarations
Acknowledgements: None.
Statement of Ethics: There is no ethical approval was obtained as it’s a case report, but written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Disclosure Statement: The authors have no conflicts of interest to declare.
References
- Von Mehren M, Randall R, Benjamin R, et al. Soft Tissue Sarcoma, Version 2. 2016, NCCN Clinical Practice Guidelines in Oncology [J]. J Nat Compr Canc Network. 2016; 14: 758-786.
- Khoubehi B, Mishra V, Ali M, et al. Adult paratesticular tumours [J]. BJU Int. 2015; 90: 707-715.
- Chiodini S, Luciani LG, Cai T, et al. Unusual case of locally advanced and metastatic paratesticular liposarcoma: A case report and review of the literature [J]. Arch Ital Urol Androl, 2015; 87: 87-89.
- Li Z, Zhou L, Zhao L, et al. Giant paratesticular liposarcoma: A case report and review of the literature [J]. Molecular and Clinical Oncology, 2018; 8: 613-616.
- Patel NG, Rajagopalan A, Shrotri NS. Scrotal Liposarcoma - a rare Extratesticular tumour [J]. JRSM Short Reports. 2011; 2: 1-3.
- Ricciotti RW, Baraff AJ, Jour G, et al. High amplification levels of MDM2 and CDK4 correlate with poor outcome in patients with dedifferentiated liposarcoma: A cytogenomic microarray analysis of 47 cases [J]. Cancer Genet. 2017; 218: 69-80.
- Li F, Tian R, Yin C, et al. Liposarcoma of the spermatic cord mimicking a left inguinal hernia: A case report and literature review [J]. World J Sung Oncol. 2013; 11: 1-5.