
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Surgical management of ear lobe keloid: A case report
Rajeev Saxena1*; Bhartendu Bharti2; Kranti Bhavna3; Vishnudas TV4
1Assistant Professor, Uttar Pradesh University of Medical Sciences, Saifai, Etawah, Uttar Pradesh, India.
2Associate Professor, ENT Department, AIIMS Patna, India.
3Professor & Head of the Department, ENT Department, AIIMS Patna, India.
4Junior resident, ENT Department, AIIMS Patna, India.
*Corresponding Author : Rajeev saxena
Assistant Professor, Uttar Pradesh University of
Medical Sciences, Saifai, Etawah, Uttar Pradesh,
India
Email: saxena.rajeev001@gmail.com
Received : Nov 01, 2023
Accepted : Nov 29, 2023
Published : Dec 06, 2023
Archived : www.jcimcr.org
Copyright : © Saxena R (2023).
Abstract
A keloid can be described as an excessive development of dense and fibrous tissue that occurs during the healing process of a skin injury. Most often occur on the chest, shoulders, upper back, back of the neck, and earlobes. Despite decades of research, the pathophysiology of keloids remains incompletely understood. Recent studies indicate that TGF-β (Transforming growth factor beta) and PDGF (Platelet-derived growth factor) play an integral role in the formation of keloids. Treatment of keloid is challenging because even after the surgical removal of the keloid there is potential risk of formation of a larger keloid in the newly traumatized area. Surgery without any adjuvant therapies can result in recurrence rates as high as 80%. The purpose of the paper is to discuss a case of keloid, review the available treatment options and recurrence rate following surgical excision with adjuvant therapy. In this case report we discuss case of 18-year-old female who presented in ENT department with complains of swelling on bilateral ear lobe in the past 9 years following ear piercing. A clinical diagnosis of keloid was made. She underwent surgical excision of keloid followed by adjuvant therapy and was followed up for recurrence. Even though various treatment options like pressure therapy, cryotherapy, radiation therapy, laser treatments are available, surgical excision followed by adjuvant therapy prove to be effective therapy in management of keloid in centres with limited resources.
Citation: Saxena R, Bharti B, Bhavna K, Vishnudas TV. Surgical management of ear lobe keloid: A case report. J Clin Images Med Case Rep. 2023; 4(12): 2723.
Introduction
Scarring is an intricate consequence of the physiological wound healing process that unfolds within the depths of the dermis. Healing cascade consists of three distinct phases i.e., inflammation, proliferation, and remodeling. After getting wounded, platelet degranulation occurs leading to cascade of events, which in turn lead to 1) formation of fibrin clot, which act as scaffold for growth of Extracellular Matrix, (ECM) 2) release and activation of cytokines & growth factors. These cytokines and growth factors act as chemotactic agent for macrophages, fibroblasts and neutrophils. Fibroblasts are responsible for formation of extracellular matrix, which in turn help in bridging of wound. Once wound get bridged excessive of ECM is degraded.
Abnormalities in scarring occur when there is a disruption in ECM protein deposition and degradation. Accumulation of ECM is enhanced by the fibro genic factors like TGF-B1 and 2 which are released from the inflammatory cells within the scar tissue. Degradation is impaired because of reduced levels of TGF B3 and MMP-9 [1]. Excessive scar formation is predisposed by the type of immune response and the severity of inflammation. Th-1 predominance attenuate fibrosis whereas Th-2 response promote fibrogenesis2 [2,3]. Compared to hypertrophic scars Keloids appear to be a more sustained and aggressive fibrotic disorder. It represent an imbalance between the anabolic and catabolic phasses [4].
A keloid can be described as an excessive development of dense and fibrous tissue that occurs during the healing process of a skin injury. This tissue growth extends beyond the confines of the initial wound site, if discernible. Unlike normal scars, keloids do not diminish naturally over time and often return after being surgically removed [5].
Keloids on the earlobe typically occur following ear piercing and, although not very common, they always lead to noticeable cosmetic and social consequences for patients. Solely relying on surgical treatment can result in recurrence rates as high as 80% [6].
Case report
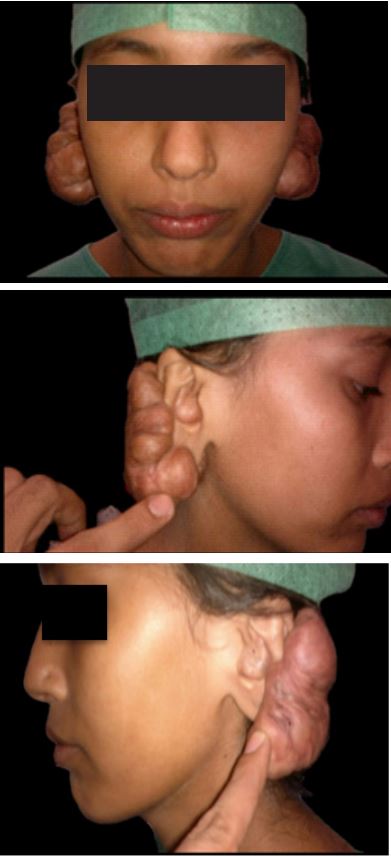
An 18-year-old girl came to the department of ENT, AIIMS Patna, with bilateral ear lobe keloids after getting ear pierced 9 years back. She had already taken a course of intralesional steroids of 6 doses but didn’t have much of an improvement (Figures 1,2,3).
She was taken up for excision of the keloid under local anesthesia. Incision was made around the keloid along the pinna. The scar tissue was completely dissected out from the skin flap and removed in-toto. The bed was checked for any residual scar tissue and vascularity of the flap was ensured. The edges were undermined and advanced to perform tension-free closure in two layers (Figures 4,5).
The scar tissue was sent for histopathological examination. Regular wound dressing were done and sutures were removed on post-operative day 7. The patient was then given injection Triamcinolone acetonide (30 mg/mL) & hyaluronidase in 1:1 ratio every week. The patient received a total of 6 doses over 2 months. Also local application of ointment Kenacort was advised to her in whole course of treatment. She was also advised to use cold compression. Follow up was done on every 3 months. The patient had a completely healthy scar and there was no evidence of recurrence of keloid till 18 months of excision (Figures 6,7).



Discussion
While keloid scars may manifest across all age groups, they exhibit a notably elevated occurrence during the second and third decades of an individual’s life. Injuries sustained by young adults appear to elicit more pronounced keloid formations in comparison to their elderly counterparts [7,8]. Keloid scars encompass not only a physical and cosmetic impediment but also entail psychological and sociological ramifications, thus exacerbating the detriment to patients’ overall well-being. These scars can induce substantial discomfort, persistent pruritus, limited range of motion, and scar contracture [9,10].
Current preventive and treatment approaches encompass pressure therapy, the use of silicone gel sheets, administration of intralesional triamcinolone acetonide, cryotherapy, radiation therapy, laser treatments, surgical excision, and proponents endorse their concurrent utilization [11]. Surgical excision of excess scar tissue creates a condition akin to a recent wound, facilitating the early application of adjunctive conservative therapies aimed at mitigating the development of renewed excessive scarring [12]. Surgical removal of the keloid may result in an elongated scar compared to the initial one, and the likelihood of keloid recurrence in this newly traumatized region could potentially result in the formation of a larger keloid. Surgery without any adjuvant therapies can result in recurrence rates as high as 80% [13-15]. Our method of delayed intralesional steroids following surgery has also been further supported by a similar trial by Donkor et al [16]. Thus by debulking of keloids by intralesional excision followed by serial injections of Triamcinolone acetonide & its local application as adjuvant therapy has proved to be an effective & promising method of management of ear lobe keloids.
Conclusion
Although management of keloid has always been a therapeutic dilemma, unavailability of extensive & advance treatment options like cryotherapy, radiation, bleomycin or interferon injections and laser treatment in rural areas has made its management more difficult. Management of keloid scar can sometimes prove to be a nightmare even for plastic surgeons as well as dermatologists. But with proper education of patient along with surgical excision and adjuvant therapy of intralesional and local application of triamcinolone and cold compresses can prove to be an effective therapy in management and prevention of recurrence of keloid in centres with limited resources.
References
- Brown JJ, Bayat A. Genetic susceptibility to raised dermal scarring. Br J Dermatol. 2009; 161: 8-18.
- Wynn TA. Fibrotic disease and the T(H)1/T(H)2 paradigm. Nat RevImmunol. 2004; 4: 583-594.
- Doucet C, Brouty-Boye D, Pottin-Clemenceau C, Canonica GW, Jasmin C, et al. Interleukin (IL) 4 and IL-13 act on human lung fibroblasts. Implication in asthma. J Clin Invest. 1998; 101: 2129-2139.
- Gauglitz GG, Korting HC, Pavicic T, Ruzicka T, Jeschke MG. Hypertrophic scarring and keloids: Pathomechanisms and current and emerging treatment strategies. Mol Med. 2011; 17: 113-125.
- Cosman B, Wolff M. Bilateral earlobe keloids. Plast Reconstr Surg. 1974; 53: 540-3.
- Cosman B, Crikelair GF, Ju DMC, Gaulin JC, Lattes R. THE SURGICAL TREATMENT OF KELOIDS: Plast Reconstr Surg. 1961; 27: 335-58.
- Bayat A, McGrouther DA, Ferguson MWJ. Skin scarring. BMJ. 2003; 326: 88-92.
- Mari W, Alsabri SG, Tabal N, Younes S, Sherif A, et al. Novel Insights on Understanding of Keloid Scar: Article Review. J Am Coll Clin Wound Spec. 2015; 7: 1-7.
- Monstrey S, Middelkoop E, Vranckx JJ, Bassetto F, Ziegler UE, et al. Updated scar management practical guidelines: Non-invasive and invasive measures. J Plast Reconstr Aesthetic Surg JPRAS. 2014; 67: 1017-25.
- Arno AI, Gauglitz GG, Barret JP, Jeschke MG. Up-to-date approach to manage keloids and hypertrophic scars: A useful guide. Burns J Int Soc Burn Inj. 2014; 40: 1255-66.
- Gauglitz GG. Management of keloids and hypertrophic scars: Current and emerging options. Clin Cosmet Investig Dermatol. 2013; 6: 103-14.
- Nast A, Eming S, Fluhr J, Fritz K, Gauglitz G, et al. German S2k guidelines for the therapy of pathological scars (hypertrophic scars and keloids). J Dtsch Dermatol Ges J Ger Soc Dermatol JDDG. 2012; 10: 747-62.
- Poochareon VN, Berman B. New therapies for the management of keloids. J Craniofac Surg. 2003; 14: 654-7.
- Robles DT, Berg D. Abnormal wound healing: Keloids. Clin Dermatol. 2007; 25: 26-32.
- Berman B, Flores F. Recurrence rates of excised keloids treated with postoperative triamcinolone acetonide injections or interferon alfa-2b injections. J Am Acad Dermatol. 1997; 37: 755-7.
- Donkor P. Head and neck keloid: Treatment by core excision and delayed intralesional injection of steroid. J Oral Maxillofac Surg Off J Am Assoc Oral Maxillofac Surg. 2007; 65: 1292-6.