
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Case report: Recurrent brain metastasis of an extremely rare benign tumor of the lung: PEComa
Murat Kara1; Berker Ozkan1; ; Hulya Yazici3; Adnan Aydiner4
1Faculty of Medicine, Department of Thoracic Surgery, Istanbul University, Istanbul, Turkey.
2Department of Pathology, Medicana International Istanbul Hospital, Istanbul, Turkey.
3Department of Genetics, Istanbul University Oncology Institute, Istanbul, Turkey.
4Department of Medical Oncology, Istanbul University Faculty of Medicine, Istanbul, Turkey.
*Corresponding Author : Eren Erdogdu
Faculty of Medicine, Department of Thoracic
Surgery, Istanbul University, Istanbul, Turkey.
Tel: + 90-505-7170960;
Email: eeren91@gmail.com
Received : Oct 17, 2023
Accepted : Nov 30, 2023
Published : Dec 07, 2023
Archived : www.jcimcr.org
Copyright : © Erdogdu E (2023).
Abstract
PEComa of the lung is a extremely rare benign tumor which originates from the perivascular epithelioid cells, which has been reported in a limited number of cases. We present a case of 58 years old woman who had a right lower lobe tumor suggesting a possible cytological diagnosis of a metastatic malignant melanoma preoperatively. The patient underwent lobectomy, and the tumor was found to be a PEComa. The patient presented with brain metastases at postoperative six months which were surgically removed. We present this unique case of a lung PEComa, which is a benign tumor, and showing brain metastases.
Keywords: Case report; Lung; Sugar tumor; PEComa; Metastasis.
Citation: Kara M, Ozkan B, Erdogdu E, Gundogdu C, Yazici H, et al. Case report: Recurrent brain metastasis of an extremely rare benign tumor of the lung: PEComa. J Clin Images Med Case Rep. 2023; 4(12): 2725.
Introduction
Perivascular epithelioid cell tumors (PEComa) also called sugar tumors or clear cell tumors of the lung are rare benign tumors, which had originally been described by Liebow and Castleman in 1963. Later, they made a review of these tumors in a series of twelve patients [1]. These particular benign lung tumors have a very high content of intracellular glycogen; thus, they are referred as sugar tumors of the lung [1].
These tumors usually react positively to both melanocytic and smooth muscle markers but no cytokeratin immunohistochemically. The differential diagnosis includes renal cell carcinoma, clear cell variant of bronchogenic carcinoma and malignant melanoma. Although benign in nature, they may show malignant behavior with vascularity and local invasion requiring a pneumonectomy [2] in addition to tumor growth either in size or number [3]. They may also appear as FDG avid tumors with high uptake [4]. Definitive preoperative diagnosis is very unlikely resulting from the rarity of these benign tumors and the above clinicopathological features.
We are aware of very few reports of PEComas of the lung in the literature [3,5]. However, we are not aware of a lung PEComa developing brain metastases. Here, we present a patient of 58 - year - old female with a right - sided tumor with high uptake of FDG. The patient underwent a right lower lobectomy with a preoperative diagnosis of malignant melanoma; however, the definitive histological diagnosis was a PEComa of the lung. Our patient is a very unique case because as having a benign tumor of the lung as PEComa, she presented with brain metastases of PEComa at postoperative six months following lung resection.
Case description
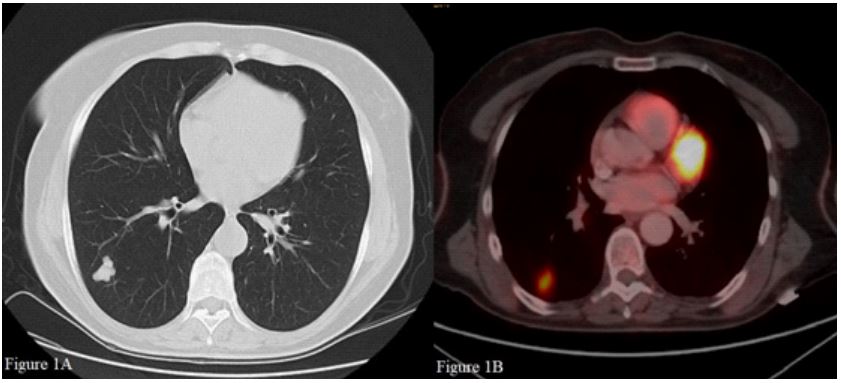
The patient was an otherwise healthy 58 - year - old woman with nonspecific chest pain who was diagnosed to have a rightsided mass on her chest x-ray during a check - up for cardiologic examination. She had no remarkable history other than medication for hypertension, and she was an ex-smoker. Physical examination and laboratory examinations did not show any abnormality. The spirometry was within the normal limits. Chest X-ray showed a pulmonary nodule at the mid - zone of the right lung. Computerized Tomography (CT) of the thorax confirmed the nodule to be located in the superior segment of the right lower lobe (Figure 1A). In addition, CT also revealed a 4 mm pulmonary nodule in the lateral basal segment of the left lower lobe and a renal stone located in the pelvis of the left kidney. Positron Emission Tomography (PET) showed that the pulmonary nodule in the right lower lobe had a maximum Standardized Uptake Value (SUVmax) of 6.9 (Figure 1B), whereas the left - sided nodule did not have any uptake. Histopathologic reading of the transthoracic fine needle biopsy was a metastasis of malignant melanoma. The cells showed strong positivity for HMB45 and weak staining for Melan – A, immunohistochemically. Diagnosis of a primary or metastatic carcinoma was excluded. The pathology report also indicated a possible clear cell sarcoma or a PEComa in the differential diagnosis. The patient underwent a thorough evaluation for a possible site of malignant melanoma. Ophthalmologic and otorhinolaryngologic examinations did not arise any suspicious lesion for malignant melanoma. Bronchoscopy did not show any endobronchial tumor and the bronchial lavage was negative for atypical cells. Colonoscopy did not show a focus consistent with malignant melanoma but only a polyp in the caecum, which was revealed to be a tubular adenoma. Gynecologic examination showed a hyperpigmented melanocytic lesion located in the left labium minus, and the histologic examination was a benign intradermal nevus.
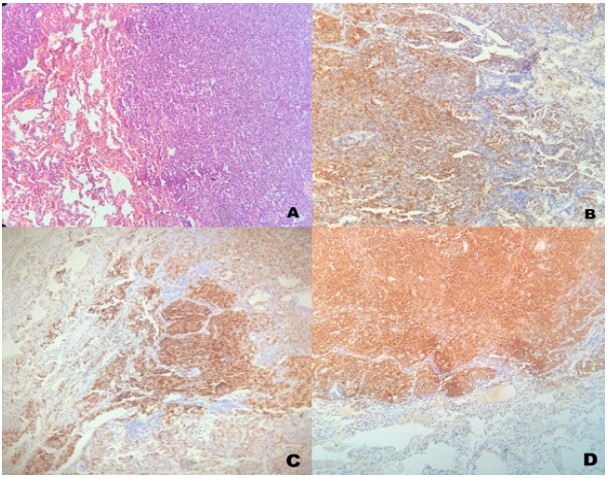
The patient underwent a videothoracoscopic right lower lobectomy and mediastinal lymph node dissection following completion of the work-up of a malignant melanoma. Macroscopically, the tumor was solid, gray, white, with irregular outer borders, and measuring 2.0 × 1.6 × 1.0 cm in the intrapulmonary location. Histopathological examination showed that the tumor consisted of organoid with thick cords and rounded nests with sinusoid-type vascular network or sheets of epithelioid cells and inconspicuous mitotic activity without any necrosis (Figure 2A). These were clear to eosinophilic granular cytoplasm, well - defined cell borders and small, uniform, rounded nuclei with small nucleoli. Immunohistochemistry showed that the tumor cells were diffuse positive for HMB-45 (Figure 2B), melan A (Figure 2C), S100 (Figure 2D) and vimentin. The tumor cells were, however, negative for cytokeratin, CK 5/6, epithelial membrane antigen (EMA), WT-1, synaptophysin, chromogranin A, inhibin, thyroid transcription factor-1, CD99, desmin, CD117 and smooth muscle actin. The KI-67 proliferation index was 40 %. All lymph nodes were negative for metastasis. The overall features favored a diagnosis of PEComa (Pulmoner Clear Cell Sugar Tumor (CCST)) of the lung. Postoperative course was uneventful, and she was discharged on postoperative day three.
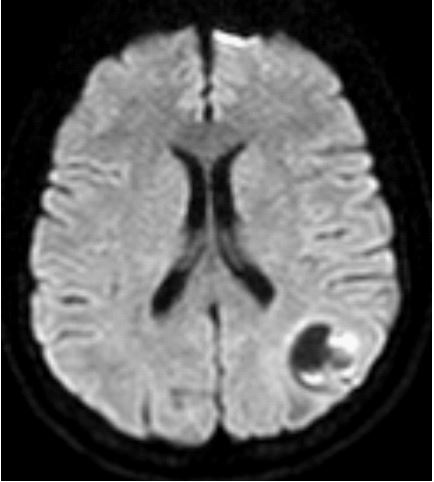
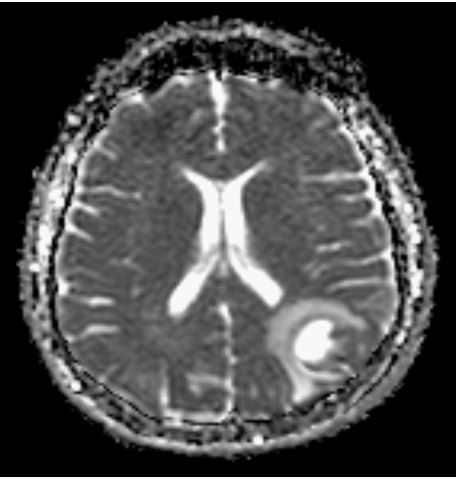
She was admitted to another hospital with syncope and hypertension attacks at postoperative six months. Her cranial magnetic resonance imaging revealed that she had two tumors, one measuring 2 cm in the left frontal lobe, and another 3.5 cm in the left posterior temporooccipital lobe (Figures 3,4). The patient underwent a craniotomy and excision of these tumors. Histology of the tumors revealed tumoral infiltration of epithelioid and spindle cells. Immunohistochemically, tumor cells were positive for S100, HMB-45, Melan- A, MITF and CD56. However, they were negative for synaptophysin, chromogranin, smooth muscle actin, desmin, TTF-1, CK 5/6, pancytokeratin, EMA, Olig2 and P40. The histological definitive diagnosis was metastases of PEComa. The patient has received radiotherapy and everolimus treatment which is a mammalian Target Of Rapamycin (mTOR) inhibitor. However, she had recurrent brain metastasis on follow-up, and she had two more operations for her metastatic tumors in the brain. She is alive with some rare epileptic seizures at postoperative 27 months.
Genetic analyses
We performed Next - Generation Sequencing (NGS) of the tumor and peripheral blood to determine the clonal origin and identify genetic cancer susceptibility. DNA and RNA samples of the Formalin-Fixed, Paraffin-Embedded (FFPE) tumor tissue and the ctDNA in the plasma of the patient were analyzed with different gene panels, on the NGS platform. In addition, in the MSI examination performed using the Microsatellite Instability testing (MSI) Analysis System Kit (Promega MD1641) in FFPE tumor tissue DNA using fragment analysis on ABI DNA Sequencer.
Results of genetic analysis
In DNA-based genetic analysis with VariantPlex CTL (ARCHER) panel; Six different pathogenic mutations were detected. Four of these mutations; c.2507C>G p.(Ser836*) mutation in APC (NM-000038.5) gene, c.832G>T p.(G278*) mutation in CDH1 (NM-004360.4) gene, c.974delC p.(Pro325Leufs*9) mutation in MET (NM-000245.3) gene, and the c.102-120delCTTGCCGTCCCAAGCAATG p.(Leu35MetfsTer3) mutation in the TP53 gene (NM-000546.5) were determined to form “stop codon”. Moreover, the c.673-1G>C mutation in the TP53 (NM-000546.5) gene caused the splice-donor error and the c.2120A>C p. (Asp707Ala) mutation in the JAK3 (NM-000215.3) gene caused the pathogenic missense mutation. It was also determined that the patient was MSS (Microsatellite stable). In the ctDNA analysis performed with the “Archer® Reveal ctDNA” gene panel in the plasma sample of the patient, 3 different changes were detected in two different genes, TP53, and NTRK3 genes. c.139C>T p.Pro47Ser and c.217G>C p.Val73Leu variants in the TP53 gene, respectively; In the NTRK3 (NC-000015.10) gene, the presence of c.2110G>A, p.Val704Ile variants were demonstrated.
In the RNA-based genetic analysis performed with the Solid Tumor Gene Fusion (ARCHER”) panel; In tumor tissue, the presence of c.61insC, p.Lys21GlnfsTer31 mutation in ETV4 (NC000017.11) gene and c.5168insA, p.Ser1723LysfsTer2 mutation in NOTCH1 (NC-000009.12) gene were detected. The gene mutations were additionally investigated in the germline DNA of the patient, since both mutations were found in the tumor tissue at a rate of 43% and 74% during the NGS analysis, respectively. It was confirmed that the gene mutations in FFPE were not found in the Germline and all mutations were proved tumor tissue specific. Pathologic mutations in tumor tissue of FFPE, and peripheral blood are shown in Table 1.
Pathogenic variants detected in the patient’s FFPE tumor tissue were determined to be tumor specific. However, there was no contribution to selecting the treatment for the patient in the databases of Onco KB (https://www.oncokb.org/), cBio Portal, CIVIC, COSMIC, Cancer Genome Interpreter (CGI), Onco Portal showing the interaction between drugs and tumor-specific variants.
Table 1: Pathologic mutations found in tumor tissue of FFPE and peripheral blood.
| Analysis | Materials | Pathogenic mutations | ||||
|---|---|---|---|---|---|---|
| RNA Based |
RNA of Tumor Tissue (FFPE) |
ETV4 (NC_000017.11) c.61insC, p.Lys21GlnfsTer31 |
NOTCH1 (NC_000009.12) c.5168insA, p.Ser1723LysfsTer2 |
|||
| DNA Based |
DNA of Tumor Tissue (FFPE) |
APC (NM_000038.5) c.2507C>G, p.(Ser836*) |
CDH1 (NM_004360.4) c.832G>T, p.(G278*) |
MET (NM_000245.3) c.974delC p.(Pro325Leufs*9) |
TP53 (NM_000546.5) c.102_120del CTTGCC- GTCCCAAGCAATG, p.(Leu35MetfsTer3) and c.673-1G>C |
JAK3 (NM_000215.3) c.2120A>C p.(Asp707Ala) |
| MSI analysis |
DNAs of Tumor Tissue (FFPE) and peripheral Blood |
Microsattellite Stable (MSS) |
||||
|
ctDNA Based (Liquid biopsy |
ctDNA of Periph- eral Blood |
TP53 (NM_000546.5) c.139C>T, p.Pro47Ser and c.217G>C, p.Val73Leu |
NTRK3 (NC_000015.10) c.2110G>A, p.Val704Ile |
|||
Discussion
We presented our case who had a preoperative diagnosis of malignant melanoma and was found to have a lung PEComa. PEComas are benign tumors that show perivascular epithelioid cell differentiation. What makes our patient a unique case is that she showed neurologic symptoms of brain metastasis at postoperative six months. The excision of these tumors proved that they were the metastasis of lung PEComa. PEComas are a family of related mesenchymal neoplasms that include angiomyolipoma, lymphangiomyomatosis, clear cell “sugar” tumor of the lung, and a group of rare, morphologically and immunophenotypically similar lesions arising at a variety of visceral and soft tissue sites [6].
These tumors mostly occur in the age group of 40 to 50 years, however the reported age ranges from 8 to 73 years. They have a slight female predominance as in our case. Patients might have hemoptysis and high fever as the rare presenting complaints. Our patient was admitted with nonspecific chest pain. However, PEComas often present as an asymptomatic pulmonary nodule without any cavitation, calcification, and lobar preference radiologically. Tumor size may differ from 1 mm to 12 cm [2,3]. They may show post-contrast enhancement in computerized tomography which might be attributed to the rich vascular stroma. Thus, they are often considered as a primary or a metastatic pulmonary tumor clinically. Positron Emission Tomography (PET) is of great clinical importance to differentiate the nature of pulmonary nodules. Although a meta-analysis comparing the diagnostic value of CT and PET-CT did not show any significant difference with respect to the diagnostic accuracy rates of either diagnostic method [7], PET-CT is a reliable and preferred imaging method, particularly for pulmonary nodules larger than 8 mm. Another meta - analysis investigating the diagnostic value of 18F-FDG-PET/CT for the evaluation of solitary pulmonary nodules revealed that its sensitivity and diagnostic accuracy rates were as high as 90 % and 93 %, respectively [8]. PEComas are benign lung tumors, thus high uptake of FDG is very unlikely. However, some cases with high uptake of FDG have been reported in the literature [4,9,10]. Among these, a huge tumor with the greatest dimension being 16 cm had an uptake of FDG as high as 46. Similarly, our patient showed a high SUVmax of 6.9.
Preoperative definitive diagnosis is a great challenge in PEComas, and it could have been established in only some cases by either a transbronchial or fine needle aspiration biopsies [3,11]. Likewise, cytological examination of the transthoracic fine needle biopsy has been interpreted as malignant melanoma in our case. Thus, the patient underwent a through entire body evaluation for a possible site of primary malignant melanoma with a resultant delay of surgical resection. Histologically, PEComas are made up of uniform, round clear cells with well-defined borders. These tumors have thin - walled vasculature with an alveolar appearance. They all share a distinctive cell type, the Perivascular Epithelioid Cell or “PEC”.
They are composed of nests and sheets of usually epithelioid but occasionally spindled cells with clear to granular eosinophilic cytoplasm and a focal association with blood vessel walls. PEComas most commonly appear to arise at visceral particularly gastrointestinal and uterine, retroperitoneal, and abdominopelvic sites, with a subset occurring in somatic soft tissue and skin. Nearly all PEComas show immunoreactivity for both melanocytic (HMB-45 and/or melan-A) and smooth muscle (actin and/or desmin) markers. However, they do not show immunoreactivity to cytokeratin and epithelial membrane antigen. The differential diagnosis should be made for metastatic renal clear cell carcinomas, clear cell carcinoid lung tumors, metastatic melanoma, granular cell tumors, oncocytoma and acinic cell tumor [12,13].
Although PEComas are considered as benign tumors and they do not show recurrence or metastasis even following an enucleation [1], however a subset of these tumors may present with malignant features. Sale et al. have reported a case with fatal recurrence and hepatic metastasis ten years following resection of a primary pulmonary PEComa [14]. Similarly, Kavunka et al. have reported a case of a PEComa showing malignant features such as vascularity and local invasion [2]. In addition, Shen et al. have reported a case with multiple tumors in the left lower lobe which showed rapid growth in size being the largest nodule as 2.8 cm and quantity from 10 to 49 in five years [3]. They emphasized the possible aggressive behavior of these benign tumors. On the other hand, Lim et al. have reported a case with enlarging multiple metachronous metastases following the removal of a large tumor measuring 12 cm in diameter 4 months after operation [15]. It has been noted that a PEComa larger than 2.5 cm with showing necrosis, marked pleomorphism and nuclear atypia should be considered for a malignant potential [13]. Similarly, the tumor in our case had some malignant features. The tumor had a high SUVmax value of on PET examination and it showed marked pleomorphism and binuclear malignant cells, histologically.
The difficulty of definitive preoperative diagnosis and the potential malignant features of PEComas make the optimal choice of treatment as surgical excision. WHO guidelines indicate the surgical excision as proper treatment, and no adjuvant therapy is recommended. However, we initiated a mTOR inhibitor in our patient because she presented with recurrent brain metastasis. Long-term survival is very likely following the excision of these tumors, however a long-term follow - up is also essential for tumors with malignant features to exclude the very low probability of a recurrence or metastasis.
Conclusion
PEComas are extremely rare benign lung tumors that may exceptionally present with malignant features. A definitive preoperative histological diagnosis might be a challenge. Tumor excision provides an adequate treatment, however tumors with malignant features might extremely present with brain metastasis on follow - up.
Declarations
Ethics Statement: Written informed consent was obtained from the patient for the publication of any potentially identifiable images or data included in this article.
Funding: The authors received no financial support for the research and/or authorship of this article.
References
- Liebow AA, Castleman B. Benign clear cell (“sugar”) tumors of the lung Yale J Biol Med. 1971; 43: 213 -22.
- Kavunkal AM, Pandiyan MS, Philip MA, et al. Large clear cell tumor of the lung mimicking malignant behavior. Ann Thorac Surg. 2007; 83: 310-2.
- Shen L, Lin J, Ren Z, Wang B, Liu Y, et al. Clear cell tumor of the lung could be aggressive: A case report and review of the literature. J Cardiothorac Surg. 2020; 15: 177.
- Zarbis N, Barth TF, Blumstein NM, Schelzig H. Pecoma of the lung: A benign tumor with extensive 18F-2-deoxy-D-glucose uptake. Interact Cardiovasc Thorac Surg. 2007; 6: 676-8.
- Olivencia-Yurvati AH, Rodriguez AE. Clear cell “sugar” tumor of the lung: Benign or malignant? Int Surg. 2015; 100: 924-926.
- Hornick JL, Fletcher CDM. PEComa: What do we know so far? Histopathology. 2006; 48: 75-82.
- Jia Y, Gong W, Zhang Z, Tu G, Li J, et al. Comparing the diagnostic value of F-FDG-PET/CT versus CT for differentiating benign and malignant solitary pulmonary nodules: A meta-analysis. J Thorac Dis. 2019; 11: 2082-2098.
- Ruilong Z, Daohai X, Li G, Xiaohong W, Chunjie W, et al. Diagnostic value of 18F-FDG-PET/CT for the evaluation of solitary pulmonary nodules: a systematic review and meta-analysis. Nucl Med Commun. 2017; 38: 67-75.
- Wu J, Jiang L, Zhang F, Huang Y, Wang H. Malignant Perivascular Epithelioid Cell Tumor of Lung on FDG PET/CT. Clin Nucl Med. 2019; 44: 469 - 471.
- Lim HJ, Lee HY, Han J, Choi YS, Lee KS. Uncommon of the uncommon: Malignant perivascular epithelioid cell tumor of the lung. Korean J Radiol. 2013; 14: 692-6.
- Takanami I, Kodaira S, Imamura T. The use of transbronchial lung biopsy to establish a diagnosis of benign clear cell tumor of the lung: report of a case. Surg Today. 1998; 28: 985-987.
- Nicholson AG. Clear cell tumor. In: Travis WD, Brambilla E, Mu ̈ller- Hermelink HK, Curtis CH, eds. WHO classification of tumors, pathology and genetics, tumors of the lung, pleura, thymous and heart. Lyon: IARC Press. 2004; 118.
- Gaffey MJ, Mills SE, Ritter JH. Clear cell tumors of the lower respiratory tract. Semin Diagn Pathol. 1997; 14: 222-232.
- Sale GF, Kulander BG. Benign clear cell tumor of lung with hepatic metastases ten years after resection of pulmonary primary tumor. Arch Pathol Lab Med. 1988; 122: 1177.
- Lim HJ, Lee HY, Han J, Choi YS, Lee KS. Uncommon of the uncommon: Malignant perivascular epithelioid cell tumor of the lung. Korean Journal of Radiology. 2013; 14: 692-6.