
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
A novel category of vasculopathy causing arterial dissection in the era of SARS-CoV-2
Faisael Albalwi1*; Gary Brahm2; Lillian Barra3
1Division of Rheumatology, Department of Medicine, King Fahad Medical City, Riyadh, Saudi Arabia.
2Division of Abdominal and Obstetrical Radiology, Clinical Lead, Body Division, Department of Medical Imaging, London Health Sciences and Western University, London, Ontario, Canada.
3Division of Rheumatology, Department of Medicine, London Health Sciences and Western University, London, Ontario, Canada.
*Corresponding Author : Faisael Albalwi
Division of Rheumatology, Department of Medicine,
King Fahad Medical City, Riyadh, Saudi Arabia.
Email: faisal1907@windowslive.com
Received : Nov 06, 2023
Accepted : Dec 04, 2023
Published : Dec 11, 2023
Archived : www.jcimcr.org
Copyright : © Albalwi F (2023).
Abstract
COVID-19 caused by the Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV-2) primarily affects the respiratory tract. However, other manifestations including vascular sequelae have been described. These vascular complications of COVID-19 are diverse and can be severe enough to cause serious complications. Moreover, some of these vascular sequelae might occur several months after the recovery of infection. SARS-CoV-2 can cause vascular pathology either via direct invasion of the endothelial layer or through a hyper-inflammatory response resulting with broad spectrum vascular insults and damage. Herein, we report a case of a 41-year-old man referred to our rheumatology clinic with suspected vasculitis who presented with renal artery dissection during a SARS-CoV-2 infection successfully treated with supportive measures. The purpose of this report is to increase awareness about a possible association between SARS-CoV-2 and severe vascular consequences.
Keywords: COVID-19; SARS-CoV-2; Infection; Arterial Dissection; Vascular Disease and Vasculopathy.
Citation: Albalwi F, Brahm G, Barra L. A novel category of vasculopathy causing arterial dissection in the era of SARS-CoV-2. J Clin Images Med Case Rep. 2023; 4(12): 2729.
Introduction
Coronavirus disease 2019 (COVID-19) is a viral infection that predominantly affects the respiratory system. However, multiple organs can be involved, including blood vessels [1].
The impact of (COVID-19) infection on the vascular tree is complex as patients might present with a broad spectrum of manifestations, such as thrombosis, dissection and long-term vascular dysfunction which might appear after a few months [2]. In this report, we present a patient diagnosed with arterial dissection in the background of (COVID-19) and review the literature regarding the effects of COVID-19 on peripheral blood vessels.
Case report and discussion about pathology
A healthy 41-year-old gentleman presented to the emergency department (ED) with a history of acute, excruciating left-sided flank pain for 2 days. Five days before, the patient developed fever, headache and malaise and he tested positive for COVID-19. The patient was previously healthy with no known prior medical conditions. He smokes 4 to 5 cigarettes per week and occassionally vapes nicotine-containing products. He drinks about 4 to 5 beers/week. He denied any history of recreational drug use and has never used intravenous drugs. The patient was unvaccinated against COVID-19 infection.
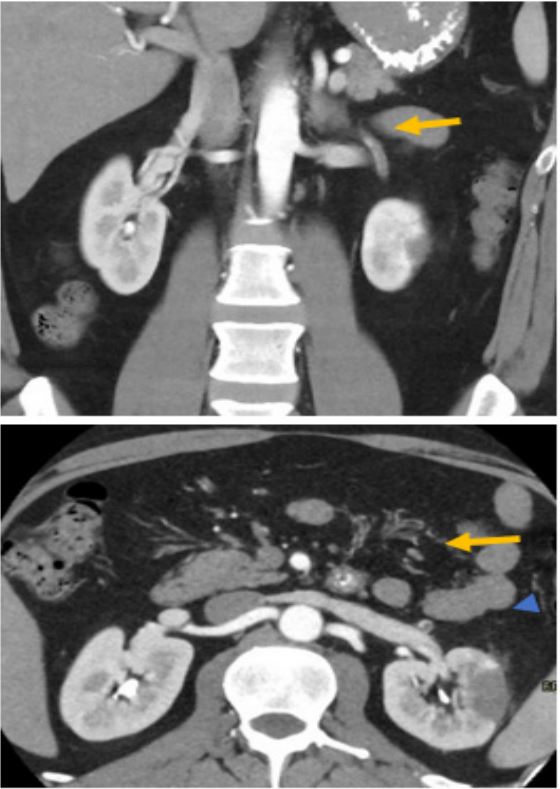
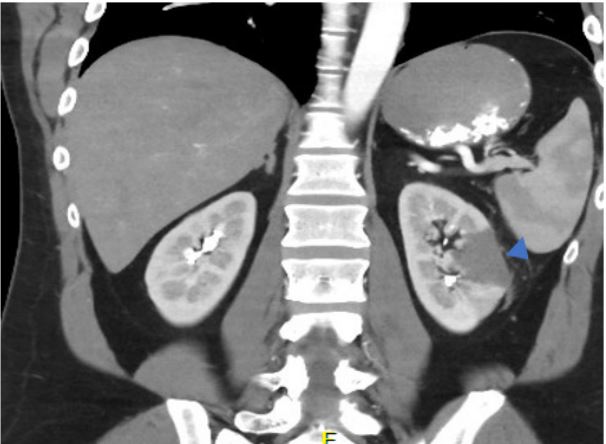
Upon arrival to the ED, he was afebrile and had high Blood Pressure (BP) 159/103 with other vitals normal. The investigations showed an elevated CRP=22.2 mg/L and a contrast-enhanced CT of the abdomen and pelvis detected an abnormality involving the left segmental renal artery with decreased opacification distally, favored to represent arterial dissection (Figure 1). An area of decreased enhancement in the lateral interpolar region of the left kidney was also present corresponding to an area of focal infarction (Figure 2). No evidence of calcified or atherosclerotic lesions. Other blood vessels were normal with no atherosclerotic disease, stenoses, thrombosis, or aneurysms. The patient was assessed by vascular surgery who recommended anti-platelet therapy with aspirin (ASA) and BP monitoring. A referral to rheumatology was made for possible vasculitis.
A comprehensive review was completed in the Interdisciplinary Vasculitis Center (IVASC) in London, Ontario. The patient had no other manifestations of vasculitis. All autoimmune and viral serologies were negative (Table 1). Screening for diabetes and dyslipidemia were negative. There was no family history consistent with hereditary collagen vascular diseases and the physical exam was unremarkable other than left flank tenderness. A CT angiogram of the head and neck and echocardiogram was unremarkable.
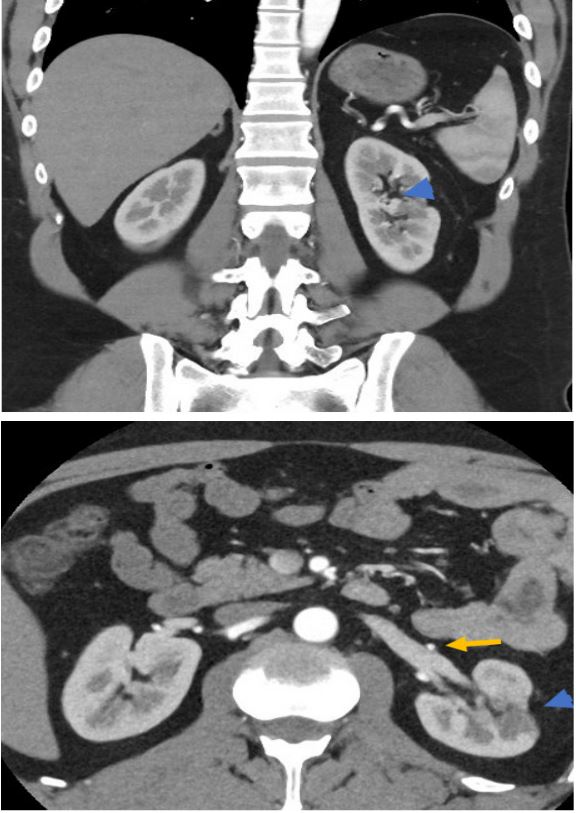
Our impression was that the patient did not have autoimmune vasculitis, connective tissue disease or collagen vascular disease. Since the dissection occurred temporally to COVID-19, we proposed that the renal artery dissection was a complication of COVID-19. At 4 months of follow-up the patient continued to be managed by the vascular surgery team with ASA therapy. His flank pain resolved completely and he has not had any additional vascular complications or new symptoms. Six months after the initial event, a repeat CT-angiogram of abdomen and pelvis revealed complete resolution of the arterial dissection and thrombosis of the anterior division of the left renal artery with small cortical thinning/scar due to focal infarct in the interpolar region of the left kidney. However, the majority of the left kidney was well perfused without evidence of ongoing ischemic changes or new arterial abnormalities (Figure 3). The patient continues to do well with no new symptoms. A written consent had been obtained from the patient directly.
COVID-19 mainly affects the respiratory tract and can cause severe complications in the lungs ranging from pneumonia, Acute Respiratory Distress Syndrome (ARDS) and Pulmonary Embolism (PE). Although SARS-CoV2 is primarily present in the respiratory tissues, it has also been identified in a variety of other organs: Gastrointestinal Tract (GI), Central Nervous System (CNS), kidneys, heart and vascular tree. One of the most devastating complications of COVID-19 is the occurrence of vascular events such as thromboembolic events, including stroke, PE and myocardial infarction [3].
SARS-CoV-2 is known to affect endothelial tissues. The endothelium is the most inner layer wrapping the blood vessels and maintaining good blood flow to different organs. A healthy endothelial layer expresses angiotensin-converting enzyme-2\ receptor (ACE) that suppresses inflammation via the release of the potent anti-inflammatory angiotensin peptide. Under physiological states, the endothelial cells protect against thrombosis by secreting thrombomodulin which participate in generating activated protein C [4].
Table 1: Laboratory investigations for our patient in (ED) upon his initial visit.
| Laboratory investigation | Reference range | Patient’s value |
|---|---|---|
| White Blood Cell Count (WBC) | 4.0-10.0 x109/L | 7.4x109/L |
| Absolute Neutrophils Count | 2.0-7.5 x109/L | 5.4 x109/L |
| Absolute Lymphocytes Count | 1.0-4.0 x109/L | 1.3 x109/L |
| Absolute Eosinophils Count | 0.0-0.4 x109/L | 0.0 x109/L |
| Hemoglobin | 135-170 g/L | 125 g/L |
| Platelets Count | 150-400 x109/L | 148 x109/L |
| Alanine Aminotransferase (ALT) | < 41 U/L | 37 U/L |
| Serum Albumin | 35-52 g/L | 40 g/L |
| Serum Creatinine | 62-120 umol/L | 77 umol/L |
| Urinalysis | Negative |
Negative for blood/protein |
| Hemoglobin A1c (HbA1c) | < 6% | 5.3% |
| Total Cholesterol | 5.20 mmol/L | 3.29 mmol/L |
| LDL-Cholesterol | <2.2 mmol/L | 1.58 mmol/L |
| Anti-Nuclear Antibody (ANA) | Negative | Negative |
|
Anti-Neutrophilic
Cytoplasmic Antibody (P/C - ANCA) |
<19 RU/mL | <2 RU/ml |
| Hepatitis-B Serology (HBsAg) | Non-Reactive | Non-Reactive |
| Hepatitis-C Serology (HCV-Ab) | Non-Reactive | Non-Reactive |
|
Human Immunodeficiency
Virus (HIV) |
Ag/Ab Screening= Non-Reactive |
Non-Reactive |
| COVID-19 Nasopharyngeal Swab | Negative | |
| Urine Culture | Negative | |
| C-Reactive Protein (CRP) | < 5 mg/L | 22.2 mg/L |
| Ferritin | 31.3-408.5 ug/L | 606.0 ug/L |
Table 2: Shows an example of some cases reported in literature about occurrence of arterial dissection around the episode of (COVID-19) infection.
| Cases | Age | Gender | Symptoms | Involved Vessels |
Timing around COVID-19 infection |
Radiological Findings |
CRP (<5 mg/L) |
Management | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| Case I (7) | 39 years |
Female |
Headache and neck pain |
Vertebral artery | 2 days |
Vertebral artery stenosis and dissection |
4 | Anticoagulation |
Improvement of symptoms |
| Case II (8) | 57 years |
Male |
Acute lower back and abdominal pain |
Splenic, Superior mesentric and Renal arteries |
1 week |
Stenosis of splenic artery with splenic and renal infarction with SMA dissection |
266 |
Anticoagulation for 6 weeks then anti- platelets therapy |
Improvement of symptoms |
| Case III (9) | 48 years |
Male |
Chest pain with heaviness |
Left anterior descending coronary artery |
3 days |
Mid-distal (LAD) dissected flap |
Not available |
Dual anti-platelets , beta- blocker and amiodarone along with diagnostic coronary angiogram |
Developed arrhythmia then improved |
| Case IV (10) | 41 years |
Male |
Severe bilateral flank pain |
Bilateral renal arteries |
5 days |
Bilateral renal arteries thrombosis with dissecting flaps |
68 |
Therapeutic catheter angiogram for kidney reperfusion with ballon angioplasty then anticoagulation , anti-platelet , statin and anti- hypertensive therapy |
Improved post therapeutic intervention |
The pathological insults responsible for damage in vascular tissues among patients with COVID-19 can be explained by various mechanisms. SARS-CoV2 bind to ACE-2\receptors, blocking their function, which subsequently leaves the inflammatory bradykinins to move freely and as a result can cause the release of pro-inflammatory cytokines like Interleukin-6 (IL-6). A state of imbalance with hypersecretion of Intracellular Adhesion Molecules (ICAM) with decreased release of Vascular Endothelial Growth Factor (VEGF) and junctional proteins is prominent in viremia due to SARS-CoV-2 disease. As a sequela of these complications, vascular integrity can be impaired with vascular leakage [5].
Vascular involvement among patients diagnosed with COVID-19 has a wide array of clinical phenotypes. The manifestations develop based on pathological changes in the wall of blood vessels. SARS-CoV-2 can cause (1) endothelial thinning and damage with degenerative changes without significant inflammatory cell infiltration (Endotheliopathy/Endotheliitis); (2) inflammatory cell deposits like neutrophilic cells in the vascular wall causing vasculitis; or (3) hyper inflammatory response (cytokinemia) which disturbs the physiological anti-thrombotic mechanism and this will lead to thromboembolism (immunethrombosis) [6].
In our case the patient developed renal artery dissection around the time of his illness with SARS-CoV-2; nevertheless, the association cannot be confirmed. The occurrence of arterial dissection in patients with COVID-19 is quite uncommon, but prior vascular events involving different territories has been reported in the literature, including cervicocranial, coronary, renal and splanchnic blood vessels based on a systematic review summarized in Table 2 [7-10].
The Management of (SARS-CoV-2) disease associated vasculopathy is dependent on a multi-disciplinary approach involving mainly the vascular surgery team and medicine subspecialties. The treatment strategy includes blood pressure control and anti-platelet /anti-coagulant therapy to prevent extensive thrombotic phenomenon. Vascular intervention is necessary when there is ischemic organ injury as reported in literature about a case with renal artery dissection during COVID-19 disease [10].
Conclusion
Vascular injury due to SARS-CoV-2 infection has a wide array of manifestations including: asculitis, vasculopathy and immune-thrombosis. All of these manifestations appear to occur most frequently around the time of COVID-19 diagnosis; however delayed-onset vascular insults might occur after months of infection. Arterial vasculopathy with dissection is a rare but possibly devastating complication of COVID-19. The management is primarily supportive, however surgical intervention is required in specific circumstances.
Conflict of Interest: None.
References
- Xu Sw, Ilyas I, Weng Jp. Endothelial dysfunction in COVID-19: An overview of evidence, biomarkers, mechanisms and potential therapies. Acta Pharmacol Sin. 2022.
- Christensen RH, Berg RMG. Vascular Inflammation as a Therapeutic Target in COVID-19 Long Haulers: HIITing the Spot? Front Cardiovasc Med. 2021; 8: 643626.
- Mokhtari T, Hassani F, Ghaffari N, Ebrahimi B, Yarahmadi A, et al. COVID-19 and multiorgan failure: A narrative review on potential mechanisms. J Mol Histol. 2020; 51: 613-628.
- Flaumenhaft R, Enjyoji K, Schmaier AA. Vasculopathy in COVID-19. Blood. 2022; 140: 222-235.
- Martínez-Salazar B, Holwerda M, Stüdle C, Piragyte I, Mercader N, et al. COVID-19 and the Vasculature: Current Aspects and Long-Term Consequences. Front Cell Dev Biol. 2022; 10: 824851.
- Becker RC. COVID-19-associated vasculitis and vasculopathy. J Thromb Thrombolysis. 2020; 50: 499-511.
- Patel P, Khandelwal P, Gupta G, Singla A. COVID-19 and cervical artery dissection- A causative association?. J Stroke Cerebrovasc Dis. 2020; 29: 105047.
- Voci D, Micieli E, Johner FA, Kucher N, Barco S. Thrombosis and Dissection of the Abdominal Arteries Associated with Infarcts of Solid Organs in a Patient with COVID-19: A Novel Clinical Entity. Hamostaseologie. 2022; 42: 195-197.
- Kumar K, Vogt JC, Divanji PH, Cigarroa JE. Spontaneous coronary artery dissection of the left anterior descending artery in a patient with COVID-19 infection. Catheter Cardiovasc Interv. 2021; 97: E249-E252.
- Parmar J, Patel T, Shah S, Kothari J, Dani S, et al. Spontaneous Renal Artery Dissection in COVID-19 Pneumonia: Potential Danger of Cytokine Storm. Case Rep Crit Care. 2021; 2021: 6696443.