
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Differentiated high grade thyroid carcinoma: Initial experience of a new entity
Faseela Beegum1*; Sandeep Vijay2 ; Vivek Nair3 ; Sithara Aravind4 ; Sangeetha Nayanar5
1Senior Resident, Department of Oncopathology & Translational Research, Malabar Cancer Centre (PGIOSR), Thalassery, Kerala, India.
2Assistant Professor, Head & Neck Surgical Oncology, Malabar Cancer Centre (PGIOSR), Thalassery, Kerala, India.
3Assistant Professor, Department of Oncopathology & Translational Research, Malabar Cancer Centre (PGIOSR), Thalassery, Kerala, India.
4Additional Professor, Department of Oncopathology & Translational Research, Malabar Cancer Centre (PGIOSR), Thalassery, Kerala, India.
5Professor and Head of Department, Department of Oncopathology & Translational Research, Malabar Cancer Centre (PGIOSR), Thalassery, Kerala, India.
*Corresponding Author : Faseela Beegum
Senior Resident, Department of Oncopathology
& Translational Research, Malabar Cancer Centre
(PGIOSR), Thalassery, Kerala, India.
Email: fasi.1989beegum@gmail.com
Received : Nov 06, 2023
Accepted : Dec 04, 2023
Published : Dec 11, 2023
Archived : www.jcimcr.org
Copyright : © Beegum FPK (2023).
Abstract
Thyroid carcinomas of follicular origin were classified as well differentiated, poorly differentiated and undifferentiated carcinomas based on their differentiation level and each group differed significantly in their prognosis. The new WHO 5th edition classification of Endocrine and Neuroendocrine tumours categorises High grade follicular cell derived malignancies of thyroid into Poorly differentiated carcinomas and High grade differentiated thyroid carcinomas, because both are characterised by high mitotic activity and necrosis with no anaplastic histology; and have intermediate prognosis. We report a case of differentiated high grade thyroid carcinoma in a 62-year-old gentlemanwithmultiple distant metastases emphasising on clinicopathologic features.
Keywords: Differentiated high grade; High grade follicular; Thyroid carcinoma.
Citation: Beegum F, Vijay S, Nair V, Aravind S, Nayanar S. Differentiated high grade thyroid carcinoma: Initial experience of a new entity. J Clin Images Med Case Rep. 2023; 4(12): 2730.
Introduction
The 5th edition of WHO classification of Endocrine and Neuroendocrine tumours (2022) has divided thyroid tumours into new categories that allow for a clearer understanding of the cell of origin, pathologic features, molecular classification and biological behaviour [1]. Thyroid follicular cell derived malignancies of high grade now includes Poorly Differentiated Carcinomas (PDTC) and High grade Differentiated Thyroid Carcinomas (DHGTC). PDTC are poorly differentiated histologically because of their solid, trabecular, and insular growth patterns [2]. DHGTC are high-grade carcinomas invasive in nature that are still differentiated because they retain the architectural or cytologic features of well-differentiated carcinomasof follicular cell origin, like architecture or nuclear features of papillary carcinoma and follicular growth pattern of follicular carcinoma [3,4].
Here we report a case of differentiated high grade thyroid carcinoma in a 62-year-old gentleman with distant metastases to the left 6th rib, iliac crest and vertebrae. To the best of my knowledge this is the first case report of this entity according to the new WHO (2022) classification of Endocrine and Neuroendocrine tumours.
Case report
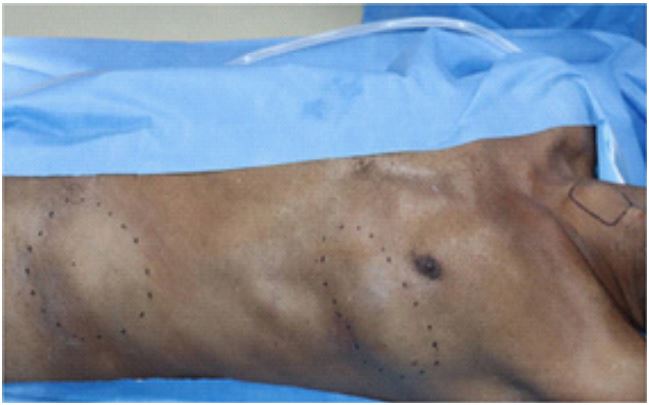
A 62-year-old gentleman presented with a swelling in the neck for 6 months and a swelling in the left hip of 2 months durationat the outpatient department of Malabar Cancer Centre, Thalassery. On Examination a left bony hard, fixed iliac swelling of size 8x5 cm, a left chest wall swelling in the 5-6th rib region measuring 5x5 cm and a thyroid swelling of size 3x3 cm were identified (Figure 1).
Ultrasonography of the neck showed a 2.9x2.6 cm heteroechoic nodule with microcalcifications in the right lobe of thyroid gland (TIRADS 5) with a metastatic right level IV node. USG guided FNAC of the thyroid nodule revealedBethesda IV (Follicular Neoplasm). FNAC of the iliac swelling showed Metastasis from Follicular neoplasm of thyroid. On further imaging a metastatic lytic lesion in the L1 vertebra was found. Based on the clinical, radiological and cytological findings a provisional diagnosis of Follicular Carcinoma Thyroid with Metastases to the neck nodes, rib, iliac crest and vertebra was made.
The case was discussed in the institutional Mult speciality tumour board. Total Thyroidectomy with Functional Neck Dissection along with resection of 6th rib and iliac crest lesion was performed and the specimens were sent to our department for histopathological examination.
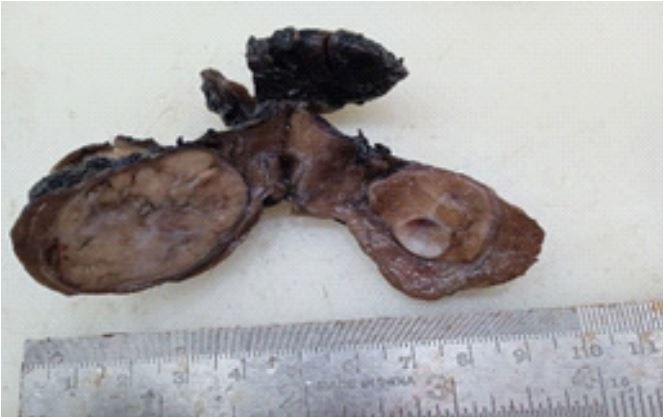
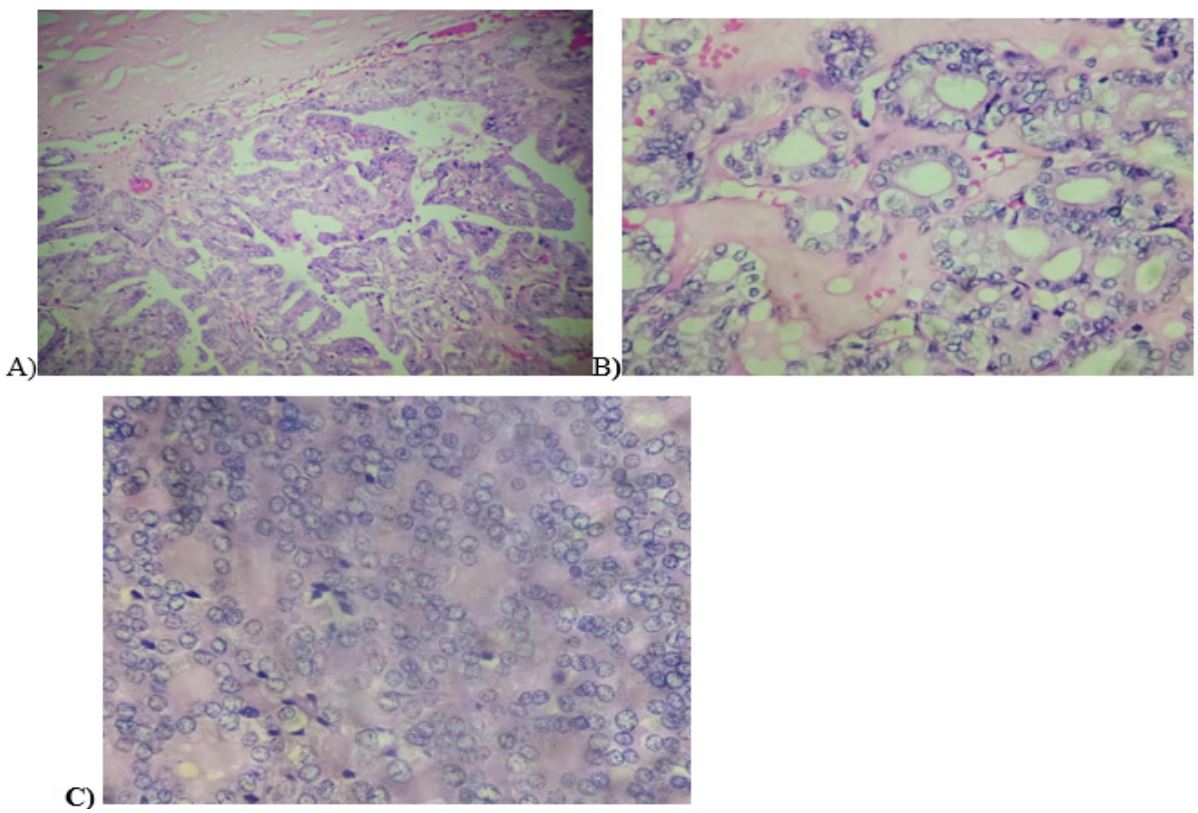
Serial sectioning through lesions in the left iliac crest and 6th rib showed grey white tumour. Hematoxylin and Eosin stained sections showed an infiltrative neoplasm with tumour cells arranged in follicular, papillary architecture and in solid sheets (Figure 4).
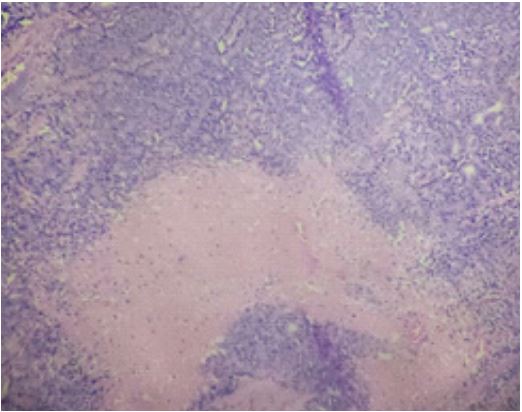
The individual tumour cells were cuboidal with moderate cytoplasm and showed nucleomegaly, overlapping, chromatin clearing and grooving.Large areas of hyalinisation, focal necrosis were also seen (Figure 5).
Focal areas of high mitotic activity 6-8/Hpf noted. Lymphovascular invasion was also seen. Extrathyroidal extension was not identified. Multiple sections studied from the left iliac crest and 6th rib showed metastatic tumours of similar histology. Two out of two lymph nodes in right level IV showed metastatic deposits. In view of the large hyalinised eosinophilic areas resembling amyloid, high mitotic count and tumour necrosis, Immunohistochemistry for calcitonin and CEA (both negative in our case) were done to rule out medullary thyroid carcinoma. Based on the current WHO classification of endocrine and neuroendocrine tumours a final diagnosis of differentiated high grade thyroid carcinoma was made.

Discussion
Differentiated high grade thyroid carcinoma is a new entity added in the 2022 classification of endocrine and neuroendocrine tumours. The new WHO classification categorises two groups of high-grade follicular cell–derived carcinomas that have intermediate prognosis. They are poorly differentiated carcinomas which are histologically poorly differentiated because of their solid, trabecular, and insular growth patterns [2]. The second one is Differentiated High-Grade Thyroid Carcinoma (DHGTC). These are invasive carcinomas that are still differentiated histologically, high-grade in nature and of follicular cell origin.
High grade carcinomas of follicular cells, both PDTC and DHGTC, share certain characteristics from clinical and epidemiological perspective. They are rare, constitute less than 1 to 6.7% of all thyroid carcinomas. Europe, and South America show higher frequencies while only few cases are reported in North America and Japan. It can be due to either ethnic or dietary factors. They usually occur in older adults over age 50 and develop as rapidly growing masses and with a female predilection [5]. Usually these tumours are often large with extrathyroidal extension and gross vascular invasion, infiltration of perithyroidal s tissues and perineural invasion. Lymph node metastases seen in almost 50% of cases [5-8]. These tumours are widely invasive grossly, but partial encapsulation are rare. Macroscopically foci of haemorrhage and tumour necrosis may be seen [5-8].
The main difference between PDTC and DHGTC are found histologically. PDTC has growth patterns like solid, trabecular or insular. In some cases, tumour cells have small dark nuclei with a convoluted appearance, which is reminiscent of papillary carcinoma nuclei [2,6]. The characteristic feature of PDTC is the presence of necrosis which appear as small or large areas of necrotic material. If tumour necrosis is absent, mitotic count should be 3 mitoses per 10 high-power fields for the carcinoma to call it as poorly differentiated. Rare PDTCs are composed of clear cells [10]. On the other hand, growth pattern in DHGTC is similar to well differentiated tumours and majority of cases showed papillary growth pattern. Nuclear features of papillary carcinoma may be present throughout, some areas of the tumour may show nuclear pleomorphism. The hallmark of DHGTC is necrosis and/or high mitotic activity (5 mitoses per 10 highpower fields/~2 mm2, 400×) [7]. Vascular, lymphatic and extrathyroidal extensions are found commonly [3,4].
Immunohistochemical stains like TTF1, PAX8, cytokeratin 7, and thyroglobulin are positive in both PDTC and DHGTC [11]. The MIB1/Ki67 proliferation index is approximately 10 to 30% [12]. Ancillary immunostains are required to exclude medullary carcinoma, parathyroid carcinoma, and metastases. Aggressive medullary thyroid carcinomas with high mitotic activity and tumour necrosis should be ruled out [13,15,16]. Immunohistochemistry for calcitonin, chromogranin, and CEA are required to distinguish them from poorly differentiated tumours of follicular cell origin. In the present case immunostaining for CEA and calcitonin were negative. Hence aggressive medullary carcinoma was ruled out.
Conclusion
Since 50 % of newly categorized high grade follicular derived tumours are resistant to conventional radioactive iodine therapy, have intermediate prognosis, they may require new treatment modalities, in particular systemic therapies focusing on molecular signature of the tumours. It is imperative that a high degree of suspicion along with concerted and meticulous effort with special emphasis on finding tumor necrosis, mitotic count and in absence of classical morphological features of poorly differentiated carcinoma are required to identify high grade areas in a conventional follicular cell derived carcinoma.
References
- Zubair W Baloch, Sylvia L Asa, Justine A Barletta, Ronald A Ghossein. C Christofer Juhlin Chan, et al. Ozgur Mete: Overview of the 2022 WHO Classification of Thyroid Neoplasms. Endocrine Pathology. 2022; 33: 27-63.
- Volante M, Collini P, Nikiforov YE, et al. Poorly differentiated thyroid carcinoma: The Turin proposal for the use of uniform diagnostic criteria and an algorithmic diagnostic approach. Am J Surg Pathol. 2007; 31: 1256-1264.
- Wong KS, Dong F, Telatar M, et al. Papillary Thyroid Carcinoma with High-Grade Features Versus Poorly Differentiated Thyroid Carcinoma: An Analysis of Clinicopathologic and Molecular Features and Outcome. Thyroid. 2021; 31: 933-940.
- Xu B, David J, Dogan S, et al. Primary high-grade non-anaplastic thyroid carcinoma: A retrospective study of 364 cases. Histopathology. 2021.
- Ibrahimpasic T, Ghossein R, Carlson DL, et al. Outcomes in patients with poorly differentiated thyroid carcinoma. J Clin Endocrinol Metab. 2014; 99: 1245-1252.
- Carcangiu ML, Zampi G, Rosai J. Poorly differentiated (“insular”) thyroid carcinoma. A reinterpretation of Langhans’ “wuchernde Struma”. Am J Surg Pathol. 1984; 8: 655-668.
- Hiltzik D, Carlson DL, Tuttle RM, et al. Poorly differentiated thyroid carcinomas defined on the basis of mitosis and necrosis: A clinicopathologic study of 58 patients. Cancer. 2006; 106: 1286-1295.
- Volante M, Landolf S, Chiusa L, et al. Poorly differentiated carcinomas of the thyroid with trabecular, insular, and solid patterns: A clinicopathologic study of 183 patients. Cancer. 2004; 100: 950-957.
- Dettmer M, Schmitt A, Steinert H, et al. Poorly differentiated oncocytic thyroid carcinoma-diagnostic implications and outcome. Histopathology. 2012; 60: 1045-1051.
- Bai S, Baloch ZW, Samulski TD, et al. Poorly differentiated oncocytic (hurthle cell) follicular carcinoma: an institutional experience. Endocr Pathol. 2015; 26: 164-169.
- Cipriani NA, Agarwal S, Dias-Santagata D, et al. Clear Cell Change in Thyroid Carcinoma: A Clinicopathologic and Molecular Study with Identification of Variable Genetic Anomalies. Thyroid. 2017; 27: 819-824.
- WHO Classification of Tumours of Endocrine Organs. Vol 10. 4th ed. Lyon, France: WHO/IARC Press.
- Kakudo K, Wakasa T, Ohta Y, et al. Prognostic classification of thyroid follicular cell tumours using Ki-67 labelling index: risk stratification of thyroid follicular cell carcinomas. Endocr J. 2015; 62: 1-12.
- Alzumaili B, Xu B, Spanheimer PM, et al. Grading of medullary thyroid carcinoma on the basis of tumour necrosis and high mitotic rate is an independent predictor of poor outcome. Mod Pathol. 2020; 33: 1690-1701.
- Fuchs TL, Nassour AJ, Glover A, et al. A Proposed Grading Scheme for Medullary Thyroid Carcinoma Based on Proliferative Activity (Ki-67 and Mitotic Count) and Coagulative Necrosis. Am J Surg Pathol. 2020; 44: 1419-1428.
- Xu B, Fuchs TL, Ahmadi S, et al. International Medullary Thyroid Carcinoma Grading System: A Validated Grading System for Medullary Thyroid Carcinoma. J Clin Oncol. 2022; 40: 96-104.