
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 4
Macular telangiectasia type 2 optical coherence tomography angiography findings
Ahmad Mirshahi1; Mojtaba Abrishami2; ; Hamid Reza Heidarzadeh2*
1Eye Research Center, Farabi Eye Hospital, Tehran University of Medical Sciences, Tehran, Iran.
2Eye Research Center, Mashhad University of Medical Sciences, Mashhad, Iran.
*Corresponding Author : Hamid Reza Heidarzadeh
Khatam-al-Anbia Eye Hospital Eye Research Center,
Mashhad University of Medical Sciences Qarani
Blvd., Mashhad 9195965919, Iran.
Tel: + 98-51- 37245363 & +98-51- 37285290;
Email: dr.hamidreza.heidarzade@gmail.com
Received : Nov 07, 2023
Accepted : Dec 05, 2023
Published : Dec 12, 2023
Archived : www.jcimcr.org
Copyright : © Heidarzadeh HR (2023).
Abstract
Purpose: To evaluate retinal vascular layers in Macular Telangiectasia Type 2 (MacTel2) imaged by Optical Coherence Tomographic Angiography (OCTA).
Methods: A prospective, observational case series study enrolled patients with MacTel2. The superficial and deep capillary plexus images were analyzed and compared to structural Optical Coherence Tomography (OCT).
Results: The study involved six patients, and 12 eyes were enrolled. The OCTA findings showed irregularities in the foveal avascular zone in both the superficial and deep plexuses. Avascular areas were also observed in the parafoveal region, along with vascular abnormalities such as telangiectatic vessels in the same area. The vascular abnormalities were more pronounced in the deep vascular plexus and were observed in areas without retinal degeneration. Additionally, the vascular changes were primarily located in the temporal parafovea.
Conclusion: Our case series documents vascular abnormalities in the normal retina, suggesting microvascular abnormalities and induced ischemic changes may precede retinal degeneration.
Keywords: Macular Telangiectasia Type 2; Optical Coherence Tomographic Angiography; Retinal degenerations.
Citation: Mirshahi A, Abrishami M, Mirghorbani SM, Heidarzadeh HR. Macular telangiectasia type 2 optical coherence tomography angiography findings. J Clin Images Med Case Rep. 2023; 4(12): 2732.
Introduction
Idiopathic perifoveal or Juxtafoveal Retinal Telangiectasia (IJRT) is a condition characterized by the abnormal dilation of small blood vessels in the retina near the center of the eye, without any apparent cause, as defined by Gass and Oyakawa [1]. Initially, the classification of this condition was based mainly on clinical examinations [1]. Later, Gass and Blodi and Yannuzzi et al. suggested a more comprehensive classification by including optical coherence tomography (OCT), high-speed indocyanine green, and fluorescein angiographic findings besides clinical examination [2,3]. IJRT can be divided into two main types: idiopathic macular telangiectasia type 1 or aneurysmal telangiectasia, which is considered a developmental, usually unilateral vascular anomaly, and idiopathic macular telangiectasia type 2 (MacTel2) or perifoveal telangiectasia, which is an acquired and bilateral condition. MacTel2 can be further categorized into a non-proliferative phase (only telangiectasia and foveal atrophy) and a proliferative phase (presence of sub-retinal neovascularization) [3]. However, Gass and Blodi classified IJRT into five stages, as follows:
1. Occult vascular abnormalities that are asymptomatic.
2. No clinically visible telangiectasis, either asymptomatic or with mild visual disturbances.
3. Prominent dilated right-angled retinal venules with metamorphopsia and mild scotoma.
4. Retinal pigment hyperplasia extending into the retina, with progressive visual decline.
5. Subretinal neovascularization with rapid and severe visual loss [2].
The incidence and prevalence of MacTel2 are still being determined since the early changes are not easily detectable, and the late changes are similar to other diseases like AMD. Therefore, it may be under-diagnosed, but it is generally considered rare [4,5]. MacTel2 usually occurs during the fifth and sixth decades, and there is no dominance in sex or race [5,6]. The pathophysiology is still not well understood, and patients typically complain of blurred vision, metamorphopsia, and positive scotoma [7-9]. During funduscopy, reduced retinal transparency with grayish discoloration is seen initially in the temporal to the fovea region, which then progresses and affects all perifovea in an oval pattern [2,3,6]. MacTel2 patients have been evaluated through various imaging modalities, including OCT, Fluorescein Angiography (FA), and Fundus Auto Fluorescence (FAF), and classified according to findings in each modality [10]. FA, which is a gold standard for the diagnosis of MacTel2, has been used for many years to study retinal vessels that show telangiectasia and dilated capillaries with dye leakage in parafoveal areas [11]. However, FA requires the injection of dye into the patient’s circulation and may not be suitable for many patients with renal failure or a history of allergy. Additionally, this modality cannot extrapolate the study to the deep retinal capillaries [12].
Optical Coherence Tomography Angiography (OCTA) is a novel diagnostic method widely investigated in various retinal pathologies. Unlike other imaging techniques, OCTA is non-invasive and does not require the injection of a dye. It provides clinicians with the ability to analyze the microvascular structure of the retina [12]. Studies conducted on OCTA in MacTel 2 patients have suggested major findings in retinal capillary plexus, which could be useful in diagnosis. However, despite its potential, more is needed to replace the currently used gold standard method of Fluorescein Angiography (FA) [10]. In our study, we used OCTA to examine 12 eyes of 6 patients with MacTel2 in order to gain a better understanding of the vascular abnormalities associated with this condition.
Methods
Study population: This observational case series study was conducted at Farabi Eye Hospital, Tehran University of Medical Sciences (TUMS), to investigate patients with MacTel2. Patients with MacTel2 and FA confirmed diagnosis obtained OCTA images of superficial and deep capillary plexus (SCP and DCP). The study and its data acquisitions were approved by the Ethical Committee of Research Deputy of Farabi Eye Hospital (Tehran University of Medical Sciences, Tehran, Iran). Patients were enrolled in the study only after providing written informed consent in compliance with the Declaration of Helsinki.
Conventional multimodal imaging: Spectral-Domain Optical Coherence Tomography (SD-OCT) (Spectralis; Heidelberg Engineering, Heidelberg, Germany) and FA (in the absence of any contraindication for fluorescein sodium injection) were performed for both eyes of study participants. Best-corrected visual acuity and refraction were also measured.
Optical coherence tomography angiography (OCTA): The instrument used for obtaining OCTA images, AngioVue, is based on Optovue RTVue XR Avanti technology. It has an A-scan rate of 70,000 scans per second and a wavelength of 840 nm. It acquires split-spectrum amplitude-decorrelation angiography images in just 3 seconds. Following this, the capillary bed is segmented and manipulated using default preset parameters.
The SCP was observed when the en-face image was segmented between two boundaries. The first boundary was 3 µm beneath the internal limiting membrane, while the second was 15 µm beneath the inner plexiform layer. To obtain the en-face image of the DCP, the inner and outer boundaries were respectively set at 15 µm and 70 µm beneath the inner plexiform layer, which resulted in a 55 µm thick slab. We also used customized thinner 24 µm slabs derived from the DCP slabs that moved progressively from the outer retina to the inner plexiform layer. Then, we preset the 20 µm choriocapillaris slab and moved it at the EZ to generate an en-face image of the ellipsoid. If a vascular signal appeared in the outer retina, we transformed the image into white and black, reinforced its contour, and superimposed it on the EZ en-face image. We recorded conventional horizontal and vertical OCT B-scans on the AngioVue device and the Spectralis (Spectralis; Heidelberg Engineering, Heidelberg, Germany).
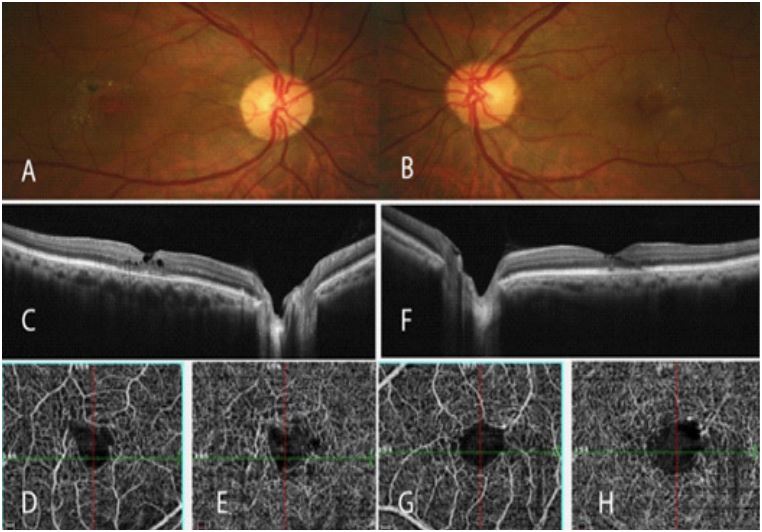
In color fundus photographs, pigmentary changes and white deposits can be seen in the foveal area (A,B). SD-OCT in the right eye shows multiple cavities in the inner and outer retinal layers in the fovea with IS/OS disruption (C). In respective OCTA images, FAZ irregularities in superficial and deep plexuses are evident (D,E). Slight similar changes can be seen in the left eye (F-H).
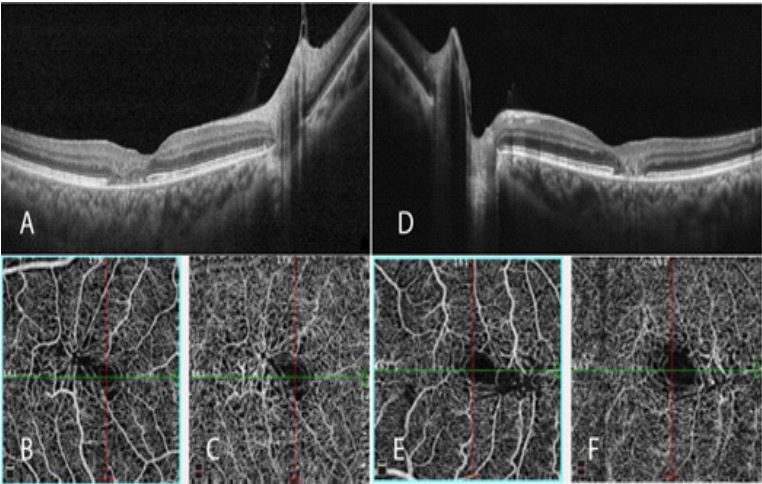
SD-OCT of both eyes shows IS/OS disruption with distorted outer retina in the fovea (A,B). Small hypo-reflective areas are seen in the outer retinal layer of the left eye. FAZ irregularities in both superficial (B,E) and Deep (C,F) plexuses of right and left eyes are more prominent in temporal parafovea. Structural changes are more pronounced in the deep plexus.
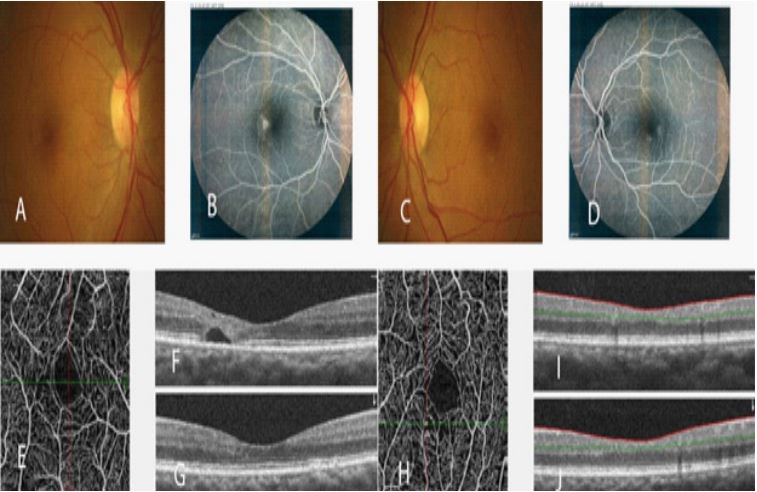
Color fundus photographs show very slight changes in the fovea in both eyes, confirmed by pinpoint hyperfluorescent dots in FA (A-D). SD-OCT in the right eye shows a hypo-reflective cavity in the outer retina in temporal parafovea compatible with temporal rarefaction seen in the OCTA (E-G). In the left eye, despite normal retinal layers in SD-OCT, parafovea rarefaction areas and telangiectatic vessels can be seen, consistent with FA findings implying early stages of the vascular disease (H-J).
Results
During the study, six patients (5 women and one man) were examined, with 12 eyes being tested. The age of the patients varied between 49 to 67 years, with an average age of 59. Two patients were initially diagnosed with branch retinal vein occlusion. However, they were not treated with anti-vascular endothelial growth factors as they did not have thickening in the macula and were referred instead. The mean visual acuity on the LogMar scale was 0.573 (approx. 20/100). Five patients had phakic eyes without any significant cataract affecting their visual acuity, whereas one was pseudophakic and experienced no complications related to the surgery.
All patients in FA exhibit perifoveal leakage accompanied by a multifocal pattern of hyperfluorescent spots. The hyperfluorescent spots were more prominent in the temporal region of the macula. SD-OCT scans showed outer retinal atrophy, mainly seen in the outer retinal nuclear layer with ellipsoid zone disruption. Cavitary retinal degeneration was observed in 9 out of 12 eyes, with the internal limiting membrane draping over the retinal degenerations.
Based on the OCTA findings, the following observations can be made. There were irregularities in the foveal avascular zone in both the superficial and deep plexuses, avascular areas were observed in the parafoveal region, and vascular abnormalities such as telangiectatic vessels in the parafovea. The vascular abnormalities were more pronounced in the deep vascular plexus and were observed in areas without retinal degenerations. These vascular changes were primarily focused in the temporal parafovea, as shown in Figures 1-3.
Discussion
MacTel2 is a bilateral progressive retinal vascular disorder where dilated vessels arise in the temporal perifoveal area and subsequently expand into the surrounding perifoveal area, causing atrophy [3,11]. The exact cause of the disease is not fully understood. However, a vascular theory was historically proposed by Gass et al., suggesting that vascular insufficiency and hypoperfusion of nutrients and oxygen to the retinal tissue lead to injury and atrophy [13]. Recent studies, however, have suggested that MacTel2 is a kind of primary neurodegenerative disease in which the Muller cells play a crucial role in abnormal processes [14-17]. These cells have been found to perform a variety of supportive functions such as balancing fluid and electrolytes, secreting cytokines and growth factors, mediating angiogenesis and anti-angiogenesis, acting as inflammatory and proliferative mediators, metabolizing neurotransmitters, facilitating synaptogenesis, and providing neuroprotection and survival for photoreceptors [18].
In a study conducted by Shen et al., it was reported that the ablation of Muller cells caused photoreceptor apoptosis, intraretinal neovascularization, and vascular telangiectasia [19]. Meanwhile, Green et al. conducted a histological study on three patients with MacTel2. They reported vascular narrowing due to the proliferation of endothelial basement membrane, along with the loss of pericytes in the posterior pole in 1980. However, they did not mention Muller cells as a contributing factor [20]. Further research by Powner et al. revealed that in the affected posterior pole area, the deep plexus of the retinal vasculature is abnormally dilated, and Muller cells are depleted [21,22].
With advancements in imaging techniques, our understanding of the disease’s pathogenesis has improved. Since MacTel2 is a microvascular abnormality, OCTA is more helpful than other modalities. Spaide et al. proposed that a cascade of retinal insults may occur not only due to the loss of Muller cells but also due to abnormal Muller cell function [18]. They used OCTA to document broad abnormalities in the deep vascular plexus in the perifoveal area in MacTel2 patients, such as thinner vessels with more expansive spaces in between and abnormal arrangements, which affect the retinal tissue’s health [18].
Our study found that in one case, vascular changes, abnormal arrangement, and rarefaction in the retina were detected by OCT imaging despite an otherwise normal appearance. OCTA imaging showed noticeable vascular changes in both superficial and deep plexuses following Spaide’s findings. The theory of ischemic changes caused by abnormal vasculature as a trigger for cascades is once again proposed. This ischemic insult may lead to Muller cell dysfunction, even if the Muller cell dysfunction is a trigger event in MacTel2 disease. Studying Muller cell populations and their functional disorders through histologic retina examination is clinically abandoned. However, identifying these vascular changes as the initial detectable findings in the natural history of MacTel2 in an otherwise normal retina is valuable. It helps predict disease progression, determine follow-up arrangements, and provide more information on the prognosis.
Our findings are consistent with previous studies on OCTA in MacTel2 patients. OCTA is superior to FA or OCT in differentiating and mapping the superficial and deep vascular plexus in retinal layers [23-26]. Moreover, OCTA is better at visualizing retinal vessel proliferation than FA [27]. In our study, all cases had irregularities in the foveal avascular zone in both superficial and deep plexuses. We also observed noticeable vascular abnormalities, such as dilated and telangiectatic vessels in the parafovea, which were more pronounced in the deep vascular plexus.
Thorell et al. were the first to apply OCTA in MacTel2 patients and concluded that abnormal perifoveal vasculature arises from the middle retinal layer [28]. Zeimer et al. reported rarefaction of the inner retinal vascular plexus, along with dilation and telangiectasis of deep retinal vascular networks [29]. Our results showed avascular areas in the parafoveal retina.
In a study conducted by Spaide et al., it was found that there was a decrease in the density of the vascular plexus in both the superficial and deep circulation. However, the reduction was more prominent in the deep circulation. The study observed decreased capillary density and the loss of functional vessels in the deep circulation. The researchers suggested that this could lead to ischemia and hypoperfusion of nutrients, resulting in the formation of new vessels and subsequent invasion of the outer and subretinal regions [18].
According to Toto et al., in a study that used quantitative vessel analysis, significant reductions were observed in both the foveal inner and outer plexus, as well as in the superficial plexus of the parafoveal region [10]. Additionally, the authors noted that in their case series study, OCTA was superior to FA in detecting neovascularization, which was also confirmed by Zhang et al. [10,27]. Vascular changes observed were predominantly focused on the temporal parafovea, consistent with the traditional classification by Gass and Oyakawa [1] and later findings in other imaging modalities [11,29,30]. This topographic distribution was also reported by Toto et al. through OCTA imaging [10]. Toto et al. compared the correlation between SD-OCT and FA, well-established modalities, and OCTA. The authors concluded that there was a high correlation not only between SDOCT and OCTA but also between FA and OCTA, which is considered the gold standard modality [10].
Based on the available data, OCTA is a non-invasive imaging tool with exceptional abilities in mapping the inner and outer plexus. It can detect both early and late stages of MacTel2 and has the potential to predict the disease’s prognosis. Using OCTA could open up new possibilities in managing retinal vascular diseases such as MacTel2. However, technical challenges are associated with this new modality, such as motion artifacts and segmentation of retinal layers. If OCTA is to be used in clinical practice, these challenges must be addressed separately. Since MacTel2 is a rare disease, studies have been conducted on a small number of patients. Therefore, conducting multicenter studies or meta-analytic reviews of previous studies would provide a more comprehensive understanding.
Declarations
Acknowledgment: Ethics approval and consent to participate: The study was conducted following the ethical standards set by the institutional and national research committee and the 1964 Helsinki Declaration, along with its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants who took part in the study.
Consent for publication: Not applicable.
Availability of data and material: The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Competing interests: The authors declare that they have no competing interests.
Funding: The authors received no funding. This is their own work, not funded by the government or academic institutes.
Authors’ contributions: All the authors contributed significantly to this research, and all authors agree to be accountable for all aspects of the work. Category 1 (a) Concept and design: AM, MA; (b) acquisition of data: MM, MA, HRH; (c) analysis and interpretation of data: all authors. Category 2 (a) drafting of manuscript: MM, MA, HRH; (b) revising it for intellectual content: all authors. Category 3 (a) final approval: all authors.
Acknowledgment: The authors would like to thank Pouran Fadakar, MSc, operator of OCTA, Roghayeh Shafei, BA and Alireza Haddadpour, BSc, Audiovisual Department, and Leyla Javdane, BSc and Maryam Nemati Soldarogh BSc, Angiography Department of Farabi Eye Hospital for their help in the process of this report. It is a pleasure for us to appreciate the kindness of Capt. Alireza Rasoulzade.
Financial disclosure: There are no financial or proprietary interests associated with any of the materials or methods mentioned, and no author has any such interests.
References
- Gass JD, Oyakawa RT. Idiopathic juxtafoveolar retinal telangiectasis. Arch Ophthalmol. 1982; 100: 769-80.
- Gass JD, Blodi BA. Idiopathic juxtafoveolar retinal telangiectasis. Update of classification and follow-up study. Ophthalmology. 1993; 100: 1536-46.
- Yannuzzi LA, Bardal AM, Freund KB, Chen KJ, Eandi CM, et al. Idiopathic macular telangiectasia. Arch Ophthalmol. 2006; 124: 450-60.
- Clemons TE, Gillies MC, Chew EY, Bird AC, Peto T, et al. Baseline characteristics of participants in the natural history study of macular telangiectasia (MacTel) MacTel Project Report No. 2. Ophthalmic Epidemiol. 2010; 17: 66-73.
- Klein R, Blodi BA, Meuer SM, Myers CE, Chew EY, et al. The prevalence of macular telangiectasia type 2 in the Beaver Dam eye study. Am J Ophthalmol. 2010; 150: 55-62 e2.
- Abujamra S, Bonanomi MT, Cresta FB, Machado CG, Pimentel SL, et al. Idiopathic juxtafoveolar retinal telangiectasis: clinical pattern in 19 cases. Ophthalmologica. 2000; 214: 406-11.
- Charbel Issa P, Helb HM, Holz FG, Scholl HP, MacTel Study G. Correlation of macular function with retinal thickness in nonproliferative type 2 idiopathic macular telangiectasia. Am J Ophthalmol. 2008; 145: 169-75.
- Charbel Issa P, Helb HM, Rohrschneider K, Holz FG, Scholl HP. Microperimetric assessment of patients with type 2 idiopathic macular telangiectasia. Invest Ophthalmol Vis Sci. 2007; 48: 3788-95.
- Charbel Issa P, Holz FG, Scholl HP. Metamorphopsia in patients with macular telangiectasia type 2. Doc Ophthalmol. 2009; 119: 133-40.
- Toto L, Di Antonio L, Mastropasqua R, Mattei PA, Carpineto P, et al. Multimodal Imaging of Macular Telangiectasia Type 2: Focus on Vascular Changes Using Optical Coherence Tomography Angiography. Invest Ophthalmol Vis Sci. 2016; 57: OCT268-76.
- Wu L, Evans T, Arevalo JF. Idiopathic macular telangiectasia type 2 (idiopathic juxtafoveolar retinal telangiectasis type 2A, Mac Tel 2). Surv Ophthalmol. 2013; 58: 536-59.
- Spaide RF, Klancnik JM, Cooney MJ. Retinal vascular layers imaged by fluorescein angiography and optical coherence tomography angiography. JAMA Ophthalmol. 2015; 133: 45-50.
- JDM G. Stereoscopic Atlas Of Macular Diseases: Diagnosis and treatment. St Louis: Mosby. 1997; 1.
- Cohen SM, Cohen ML, El-Jabali F, Pautler SE. Optical coherence tomography findings in nonproliferative group 2a idiopathic juxtafoveal retinal telangiectasis. Retina. 2007; 27: 59-66.
- Koizumi H, Cooney MJ, Leys A, Spaide RF. Centripetal retinal capillary proliferation in idiopathic parafoveolar telangiectasis. Br J Ophthalmol. 2007; 91: 1719-20.
- Koizumi H, Slakter JS, Spaide RF. Full-thickness macular hole formation in idiopathic parafoveal telangiectasis. Retina. 2007; 27: 473-6.
- Olson JL, Mandava N. Macular hole formation associated with idiopathic parafoveal telangiectasia. Graefes Arch Clin Exp Ophthalmol. 2006; 244: 411-2.
- Spaide RF, Klancnik JM, Jr., Cooney MJ. Retinal vascular layers in macular telangiectasia type 2 imaged by optical coherence tomographic angiography. JAMA Ophthalmol. 2015; 133: 66-73.
- Shen W, Fruttiger M, Zhu L, Chung SH, Barnett NL, et al. Conditional Mullercell ablation causes independent neuronal and vascular pathologies in a novel transgenic model. J Neurosci. 2012; 32: 15715-27.
- Green WR, Quigley HA, De la Cruz Z, Cohen B. Parafoveal retinal telangiectasis. Light and electron microscopy studies. Trans Ophthalmol Soc U K. 1980; 100: 162-70.
- Powner MB, Gillies MC, Tretiach M, Scott A, Guymer RH, et al. Perifoveal muller cell depletion in a case of macular telangiectasia type 2. Ophthalmology. 2010; 117: 2407-16.
- Powner MB, Gillies MC, Zhu M, Vevis K, Hunyor AP, et al. Loss of Muller’s cells and photoreceptors in macular telangiectasia type 2. Ophthalmology. 2013; 120: 2344-52.
- Fingler J, Zawadzki RJ, Werner JS, Schwartz D, Fraser SE. Volumetric microvascular imaging of human retina using optical coherence tomography with a novel motion contrast technique. Opt Express. 2009; 17: 22190-200.
- Jia Y, Tan O, Tokayer J, Potsaid B, Wang Y, et al. Split-spectrum amplitude-decorrelation angiography with optical coherence tomography. Opt Express. 2012; 20: 4710-25.
- Mendis KR, Balaratnasingam C, Yu P, Barry CJ, McAllister IL, et al. Correlation of histologic and clinical images to determine the diagnostic value of fluorescein angiography for studying retinal capillary detail. Invest Ophthalmol Vis Sci. 2010; 51: 5864-9.
- Motaghiannezam SM, Koos D, Fraser SE. Differential phase-contrast, swept-source optical coherence tomography at 1060 nm for in vivo human retinal and choroidal vasculature visualization. J Biomed Opt. 2012; 17: 026011.
- Zhang Q, Wang RK, Chen CL, Legarreta AD, Durbin MK, et al. Swept Source Optical Coherence Tomography Angiography of Neovascular Macular Telangiectasia Type 2. Retina. 2015; 35: 2285-99.
- Thorell MR, Zhang Q, Huang Y, An L, Durbin MK, et al. Sweptsource OCT angiography of macular telangiectasia type 2. Ophthalmic Surg Lasers Imaging Retina. 2014; 45: 369-80.
- Zeimer M, Gutfleisch M, Heimes B, Spital G, Lommatzsch A, et al. Association between Changes in Macular Vasculature in Optical Coherence Tomography- and Fluorescein- Angiography and Distribution of Macular Pigment in Type 2 Idiopathic Macular Telangiectasia. Retina. 2015; 35: 2307-16.
- Sallo FB, Leung I, Clemons TE, Peto T, Bird AC, et al. Multimodal imaging in type 2 idiopathic macular telangiectasia. Retina. 2015; 35: 742-9.