
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Implantable cardioverter defibrillator malfunction and pocket infection due to blunt trauma from gunshot wound
Gurjap Singh Dhaliwal, MD*; Avinash Sharma, MD; Brandon Woodbury, MD
Ross University School of Medicine, USA.
*Corresponding Author : Gurjap Dhaliwal
Ross University School of Medicine, USA.
Email: gurjap_dhaliwal@yahoo.com
Received : Nov 08, 2023
Accepted : Dec 06, 2023
Published : Dec 13, 2023
Archived : www.jcimcr.org
Copyright : © Dhaliwal G (2023).
Abstract
We present an uncommon cause for Implantable Cardioverter Defibrillator (ICD) pocket infection. Penetration of the ICD pocket from a gunshot wound resulted in blunt trauma to the ICD, and its malfunction. The ICD was removed and we highlight post-procedural management of this rare clinical scenario.
Citation: Dhaliwal GS, Sharma A, Woodbury B. Implantable cardioverter defibrillator malfunction and pocket infection due to blunt trauma from gunshot wound. J Clin Images Med Case Rep. 2023; 4(12): 2734.
History of presentation
This is a 61-year-old male with a past medical history of bipolar disorder, Coronary Artery Disease (CAD), heart failure with reduced ejection fraction of <20% (HFrEF) s/p Biotronik ICD placement in 2019 for primary prevention, and polysubstance abuse who presented to the ED after multiple Gunshot Wounds (GSW) to the chest and arms. On presentation, he denied dyspnea, chest pain, palpitations, orthopnea; however, he endorsed pain at the site of his GSWs. On physical examination, his vital signs were within normal limits. Two GSWs to the left anterior chest were noted with an entry and exit wound that were superficial and over the ICD, with the bullet exiting laterally and not through the thorax. In addition, one GSW in the left upper arm was noted that was also superficial with no significant deep injuries. An attempt to interrogate the ICD was performed, however no radio frequency signal was obtained. Therefore, it was believed the device was nonfunctional.
Medical history
Our patient’s medical history includes several acute heart failure exacerbations with prior negative non-invasive ischemic workups. Our patient has a history of polysubstance abuse with methamphetamine, cocaine and marijuana use. Given this clinical picture, it was believed the etiology of his cardiomyopathy was non-ischemic and due to substance abuse. He was on Guideline Directed Medical Therapy (GDMT), however, with no improvement in left ventricular systolic function, an ICD was implanted for primary prevention. Before and after its implantation, our patient did not endorse any arrhythmia history and did not require any cardioversion or defibrillation.
Differential diagnoses
ICD that was end of life (EOL)
ICD malfunction due to blunt trauma
ICD pocket infection from exposed generator
Investigations
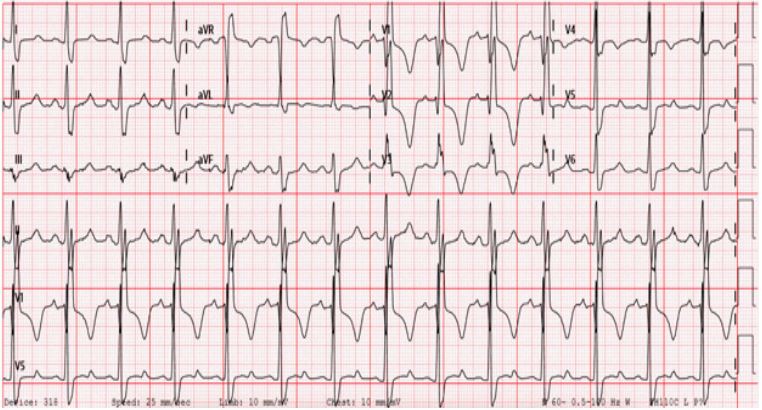
Electrocardiogram was notable for normal sinus rhythm and a right bundle branch block (Figure 1). Initial pertinent laboratory values included a normal hemoglobin 13.7 g/dL and platelets 231 x 109 cells/L, as well as a normal troponin I. B-type natriuretic peptide was elevated at 1508 pg/ml. Urine drug screen was positive for methamphetamine and cannabis.
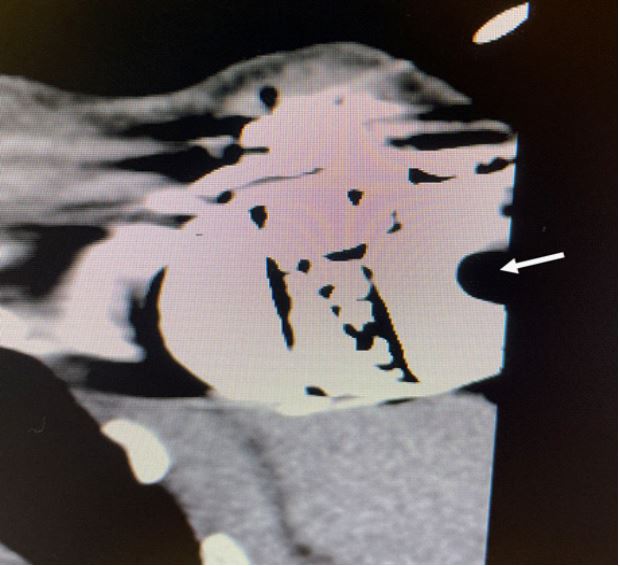
Imaging was performed with an initial X-ray of the left humerus revealing no fracture or retained foreign body/bullet fragments. Chest X-ray revealed left sided ICD with mildly enarged cardiac silhouette. Further imaging with CT chest showed cardiac enlargement, emphysematous changes, and an ICD with defects on its surface consistent with blunt trauma from GSW (Figure 2). Recent echocardiogram was significant for known severe left ventricular systolic dysfunction with an ejection fraction <20%, mild right ventricular dilation and normal function, moderate bi-atrial enlargement, moderate to severe mitral and tricuspid regurgitation, and severely elevated pulmonary artery systolic pressures of 60-70 mmHg. These echocardiographic findings were similar to prior studies.
Culture of the ICD pocket grew Staphylococcus aureus.
Management
The patient’s GSWs were evaluated by our trauma team, and were deemed superficial with no operative intervention needed. The wounds were irrigated and treated with dry dressings. He was transferred to the medicine team where GDMT was reinitiated for his HFrEF, which included diuretics. As mentioned above, ICD interrogation was notable for a non-functional device from traumatic injury due to extensive damage to the ICD’s generator from GSWs.
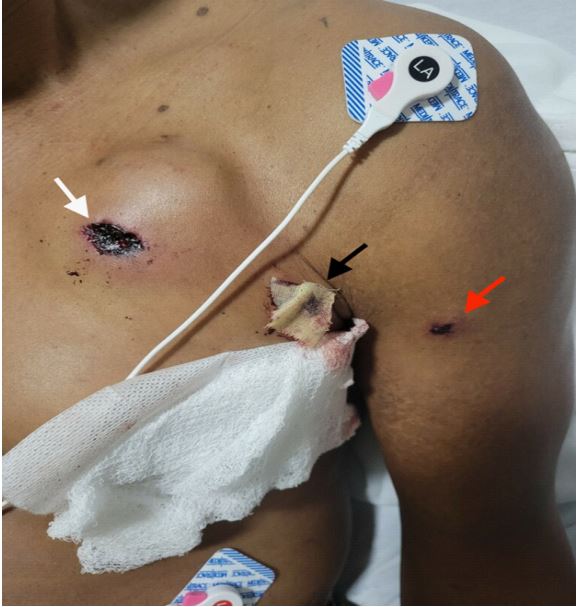
The ICD’s pocket was compromised with non-sterile material (i.e. a bullet). The bullet entered over the device and exited laterally, creating a tract and damaging the generator with blunt trauma (Figure 3). Given the introduction of non-sterile material into the pocket, it was determined that both the device and pocket were infected. As the ICD was implanted for primary prevention and the patient did not require any pacing from the device, we planned for removal of the device with a device free time period and antibiotics prior to re-insertion. We planned for laser assisted extraction with removal of the ICD leads and generator
The patient was brought to the Electrophysiology (EP) suite and we proceeded with extraction under general anesthesia with transesophageal guidance. Vascular access was obtained with 5 French arterial and venous sheaths placed in the right femoral artery in case of hemodynamic comprising needed resuscitation and/or upsizing to mechanical circulatory support. Incision was performed over the prior generator scar and was carried down with electrocautery and blunt dissection. Sterile culture swabs were taken from the pocket. Next the generator was removed, and a centimeter indentation was noted over the device on the lateral aspect. After, attention was taken to the leads which were removed with the use of laser assisted removal tools. Upon successful removal of the entire ICD (generator and leads), the pocket was inspected. The inferolateral portions of the pocket revealed pieces of shrapnel, which were then removed. Fluoroscopy confirmed adequate removal of the shrapnel with no remaining fragments. A skin fistula with seepage of irrigation material was also noted at the inferolateral portion of the pocket where the bullet had exited. The pocket did not show any clinical signs of infection but was irrigated with an antibiotic solution. The pocket was closed with three running layers of absorbable suture. Staples were placed for skin closure and surgical dressings were then applied. Postoperative antibiotics were given.
The patient tolerated this procedure well, and was discharged on postoperative day 1. The sterile wound cultures taken during ICD extraction grew methicillin sensitive Staphylococcus aureus. Blood cultures did not grow any organisms and there were no echocardiographic findings of infection. With the device removed and no clinical signs of infection in the pocket or systemic findings of an infection, the patient was discharged without systemic antibiotics. The patient had inpatient intravenous antibiotics before and after the ICD extraction.
Discussion
At the time of the first ICD implantation in 1980 [1], the large device size warranted an open thoracotomy for device placement. With the evolution of technology, ICD sizes generally decreased to the point where an open thoracotomy was no longer required and the placement of an ICD was achieved via a prepectoral approach. This resulted in a decreased incidence of pocket infections after ICD placement to <7% [1]. Despite the advancement in technology and surgical techniques to place an ICD, the incidence of ICD infections has surpassed the number of actual ICD placements [1].
The risk factors for a Cardiovascular Implantable Electronic Device (CIED) infection can be broken down into patient and device specific risk factors [1]. Patient specific risk factors include younger age, chronic kidney disease with or without dialysis, valvular disease, congestive heart failure, chronic obstructive pulmonary disease, atrial fibrillation, immunosuppression therapy, anticoagulation, and possibly male gender. Device related risk factors include additional manipulation to an already implanted device, using an epicardial or extrathoracic approach as compared to a transvenous approach for ICD placement, and the presence of extra leads.
The most commonly isolated organisms in 60-70% of ICD pocket infections are Staphylococcus aureus and Coagulase negative Staphylococci. Because these organisms can produce biofilm, the most effective management for a suspected pocket infection is removal of the entire device, including the leads. Percutaneous methods are preferred for infected lead removal followed by removal of the generator. Cardiothoracic surgery is only indicated if there is a large lead vegetation (>20mm) or if the patient is undergoing cardiac surgery for other reasons [2]. Intraoperative ICD pocket irrigation with bacitracin, vancomycin, or a cephalosporin should suffice for Staphylococcus aureus and Coagulase negative Staphylococci coverage [3] and post-procedural antibiotic therapy is generally preferred for 10- 14 days. Conservative management has been explored, which includes the use of a vacuum assisted wound closure system, but more research needs to be done [3].
Reimplantation of a device after a pocket infection requires medical justification for further need of the CIED. If reimplantation is clinically indicated and necessary, it should be undertaken once systemic symptoms are absent. The ideal time for reimplantation is not known but some studies have suggested a 7-10 day window for device reimplantation [2,3]. If immediate reimplantation of a device is necessary, a new site for implantation is recommended [4-10].
Follow up
Following hospital discharge, the patient was followed closely outpatient for heart failure management. He did not have any hospitalizations, re-admissions, or events requiring ICD/defibrillation. A dual-chamber ICD was re-implanted 6 months after his pocket infection. The patient continues to do well.
Conclusion
CIED pocket infections are seen in clinical practice from a variety of causes. We present a rare case of this occurring after blunt trauma from a GSW which exposed the pocket and damaged the ICD generator, resulting in its malfunction. Timing of device re-implantation after a pocket infection can be challenging, and the risks/benefits including the indication of the CIED should be taken into account.
Learning points: (1). Device pocket infections can occur due to a variety of reasons, and removal should be weighed against the risks/benefits of removal including initial indications for device placement. (2). Blunt trauma to a CIED can result in its malfunction, this can also occur, albeit rarely, from GSW.
References
- Mirowski M, Reid PR, Mower MM, Watkins L, Gott VL, et al. Termination of malignant ventricular arrhythmias with an implanted automatic defibrillator in human beings. N Engl J Med. 1980; 303: 322-324.
- Mela T, McGovern BA, Garan H, Vlahakes GJ, Torchiana DF, et al. Long-term infection rates associated with pectoral versus abdominal approach to cardioverter-defibrillator implants. Am J Cardiol. 2001; 88: 750-753.
- Prutkin JM, Reynolds MR, Bao H, Curtis JP, Al-Khatib SM, et al. Rates of and factors associated with infections in 200909 Medicare Implantable cardioverter defibrillator implants. Circulation. 2014; 130: 1037-1043.
- Hui-Chen Han, Nathaniel M Hawkins, Charles M Pearman, David H Birnie, Andrew D Krahn. Epidemiology of cardiac implantable electronic device infections: Incidence and risk factors, EP Europace. 2021; 23: iv3-iv10.
- Jonathan AT Sandoe, Gavin Barlow, John B Chambers, Michael Gammage, Achyut Guleri, et al. Guidelines for the diagnosis, prevention and management of implantable cardiac electronic device infection. Report of a joint Working Party project on behalf of the British Society for Antimicrobial Chemotherapy (BSAC, host organization), British Heart Rhythm Society (BHRS), British Cardiovascular Society (BCS), British Heart Valve Society (BHVS) and British Society for Echocardiography (BSE). J Antimicrobial Chemotherapy. 2015; 70: 325-359.
- Zheng Q, Di Biase L, Ferrick KJ, Gross JN, Guttenplan NA, et al. Use of antimicrobial agent pocket irrigation for cardiovascular implantable electronic device infection prophylaxis: Results from an international survey.
- Sekiguchi Y. Conservative therapy for the management of cardiac implantable electronic device infection. J Arrhythm. 2016; 32: 293-296.
- Ipek EG, Guray U, Demirkan B, et al. Infections of implantable cardiac rhythm devices: Predisposing factors and outcome Acta Cardiol. 2012; 67: 303-10.
- Catanchin A, Murdock CJ, Athan E. Pacemaker infections: A 10-year experience Heart Lung Circulation. 2007; 16: 434-9.
- Larry M Badddoir, Andrew E Epstein, Christopher C Erickson, Bradley P Knight, Matthew E Levison, et al. Council on Cardiovascular Surgery and Anesthesia, Coucil on Cardiovascular Nursing, Council on Clinical Cardiology and the Interdisciplinary council on Quality of Care and Outcomes Research and on behalf of the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee of the Council on Cardiovascular Disease in the Young. Ciruculation. 2010; 121: 4558-477.