
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Bilateral Grynfeltt lumbar hernia: A rare case report
Tien Tran Phung Dung; Huan Nguyen Ngoc*; Trung Lam Viet
Digestive Surgery Department, Cho Ray Hospital, Vietnam.
*Corresponding Author : Huan Nguyen Ngoc
Digestive Surgery Department, Cho Ray Hospital,
Vietnam.
Email: ngochuan1710@gmail.com
Received : Nov 12, 2023
Accepted : Dec 08, 2023
Published : Dec 15, 2023
Archived : www.jcimcr.org
Copyright : © Nguyen Ngoc H (2023).
Abstract
Introduction: Lumbar hernias are rare, with only around 300 cases reported in the literature. The posterolateral abdominal wall has two weak areas, the superior (Grynfeltt-Lesshaft’s triangle) and the inferior (Petit’s triangle) lumbar triangles, where superior and inferior lumbar hernias can occur. These hernias pose a diagnostic and therapeutic challenge to most surgeons due to their rarity. Computed tomography is the gold standard for confirming the diagnosis, based on clinical findings. The treatment of lumbar hernia has various approaches, both open and laparoscopic, but the optimal method for each patient is still debatable. We opted for an open repair with retro-muscular polypropylene mesh placement, which is an affordable technique in Cho Ray hospital. Our aim is to raise awareness of superior lumbar hernias and to discuss surgical repair options.
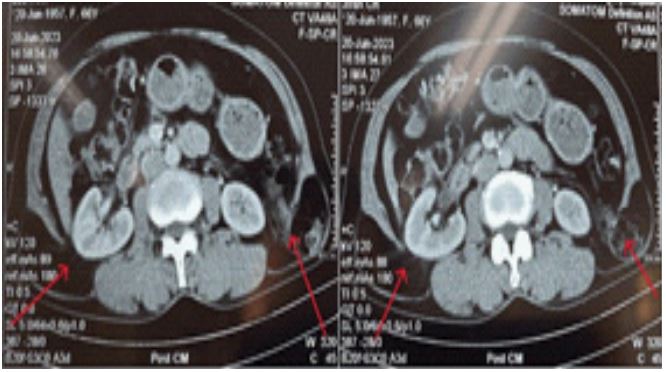
Case presentation: We report a case of a 66-year-old woman who presented with bilateral lumbar masses that had been present for 3 years. She had no history of trauma or surgery. The masses were soft, painless, and reducible, and they increased in size with coughing or straining. They were not pulsatile and measured 2 x 2 cm on the right and 3 x 4 cm on the left. Ultrasound and CT scan of the upper lumbar region showed two lipomatous masses protruding through Grynfeltt’s quadrilateral on both sides. The diagnosis of bilateral Grynfeltt hernia was made and herniorrhaphy was advised. The herniated retroperitoneal and omental fat was repositioned, and the abdominal wall defect was repaired with retro-muscular mesh, which was sutured to the fascia. The postoperative course was uneventful, and the patient was discharged 48 hours after the surgery.
Conclusion: Grynfeltt-Lesshaft hernia is a rare surgical condition that results from a congenital or acquired defect in the posterior lumbar wall. It may present with lower back pain or a localized tender point over the hernia, as well as a lumbar mass that disappears when lying down. Open repair remains a safe and effective option for this condition.
Keywords: Hernia; Lumbar hernia; Bilateral Grynfeltt.
Citation: Phung Dung TT, Nguyen Ngoc H, Lam Viet T. Bilateral Grynfeltt lumbar hernia: A rare case report. J Clin Images Med Case Rep. 2023; 4(12): 2738.
Introduction
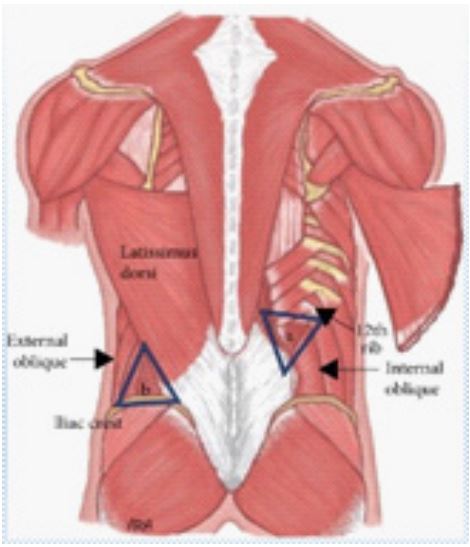
Lumbar hernias are uncommon surgical conditions, with only 300 cases reported in the literature [1]. They represent less than 1.5% of all abdominal hernias [2]. The lumbar region has two boundaries: superiorly by the twelfth rib, inferiorly by the iliac crest, medially by the erector spinal muscles, and laterally by the external oblique muscle. There are two weak areas: the inferior lumbar triangle (Jean-Louis Petit triangle) and the superior lumbar triangle (Grynfeltt-Lesshaft triangle). The Grynfeltt-Lesshaft triangle is an inverted triangle, delimited by the twelfth thoracic rib superiorly, the erector spinal muscle group medially, and the internal oblique muscle laterally (Figure 1). The transversal muscle aponeurosis forms the base of this triangle, and the latissimus dorsi muscle forms the cover [3]. Most lumbar hernias are unilateral, but some rare cases of bilateral lumbar hernias have been reported. Lumbar hernias are seldom encountered and managed by general surgeons, so a high index of suspicion is needed to diagnose them and plan proper treatment to avoid the significant risk of complications. About 25% of cases may become incarcerated and 8% strangulated [2].
Lumbar hernias often cause low back pain, but their clinical diagnosis is challenging due to non-specific symptoms. There is no agreement on the optimal method for lumbar hernia repair. We present a case of bilateral Grynfeltt lumbar hernia in the Digestive Surgery Department of Cho Ray Hospital.
Case presentation
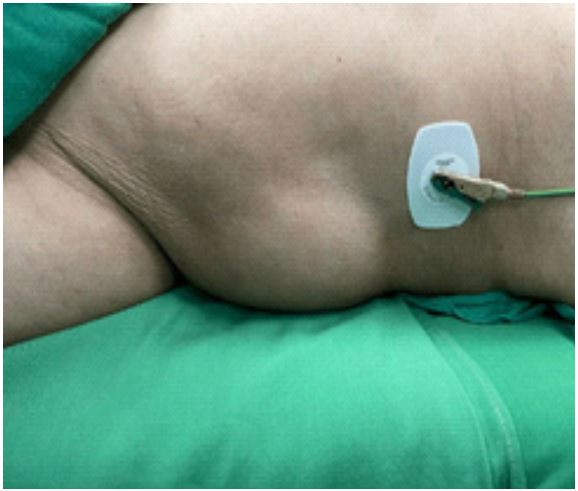
We show a case of a 66-year-old woman who presented with bilateral painful lumbar masses that had been present for three years. She has married and worked as a farmer for several years. She initially noticed a mass in the Grynfeltt area without any pain or vomiting. She did not seek any medical attention and had no previous surgery. However, after several months, she was diagnosed with bilateral lumbar hernia. The masses were soft, painless, and reducible. They measured 3 x 4 cm on the right side and 2 x 2 cm on the left side. They increased in size with coughing or straining (Figure 2).
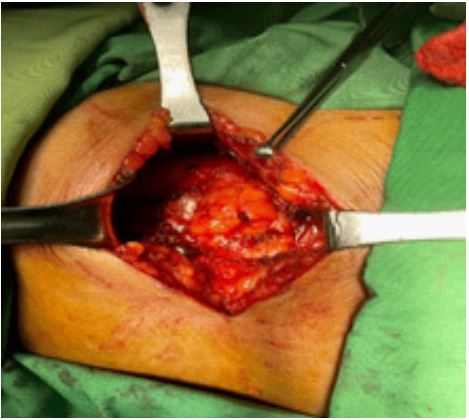
We performed pre-operative evaluations and obtained informed consent, and then operated on the patient under general anesthesia in the left lateral position. We made a 10 cm transverse incision on the protruding area, and after dissecting the skin, subcutaneous tissue, and muscle layer (latissimus dorsi), we encountered a hernia sac through a 3 cm defect. The sac contained herniated retroperitoneal fat, which we repositioned and repaired the abdominal wall defect with retro-muscular or sublay Monofilament Polypropylene Mesh (Figure 4).
We sutured the mesh to the fascia with non-absorbable interrupted sutures using a tension-free technique (Figure 5).
We closed the muscles and fascia separately with absorbable sutures, and the wound. We did not need a drain catheter. After completing the left side, we changed the patient’s position, and repeated the same procedure on the right side, where we found a hernia sac of 2.0 cm. The total operative time was 130 minutes, and the patient had no postoperative complications during the hospital stay. The patient was discharged 48 hours after the surgery with satisfactory outcomes.

Discussion
Lumbar hernias are rare acquired or congenital conditions. They are often misdiagnosed as lipomas because of their rarity and non-specific symptoms, such as low back pain and a lumbar mass that disappears when lying down [5]. The mass may start small and gradually enlarge. Patients are usually between 50 to 70 years old [3]. Because lipomas and lumbar hernias have similar presentations, doctors should consider other possible diagnoses, such as abscesses, hematomas, or soft tissue tumors. The hernia content can be kidney, retroperitoneal fat, colon, omentum, appendix, small bowel, ovary, or spleen [6]. In obese patients, identifying the mass is particularly difficult. Our patient had an acquired hernia with protrusion of retroperitoneal fat. Surgical repair is necessary to correct the defect and reconstruct an abdominal wall that is both elastic and resistant to daily physical stress [7]. The risk of strangulation should always be indicated, especially when intestinal content is involved. Several techniques have been described in the literature, but the most common methods are open and laparoscopic approaches. There is no consensus on the best way to repair a lumbar hernia because of its rarity. Laparoscopic repair of lumbar hernias has many advantages, such as less pain, minimal invasiveness, shorter stay at hospital, and faster recovery. However, most surgeons are not familiar with the laparoscopic view of the lumbar area for this rare hernia, so advanced laparoscopic skill and experience are required [8]. The open approach is the most popular technique and is safe, effective, and affordable. Our patient underwent open technique to bilateral hernia repair with retromuscular using polypropylene mesh.
Conclusion
Grynfeltt-Lesshaft hernia is a difficult condition to diagnose because it is a rare one with both congenital and acquired causes and it presents as lower back pain and a lumbar mass that disappears when lying down. While a CT scan is the best method for diagnosis, it may not be accessible to all patients. Open repair is still a safe and effective option. The choice of surgical repair depends on the size of the fascial defect and the surgeon’s expertise.
References
- AlAli MN, et al. Bilateral fat containing lumbar hernia © Am J Case Rep. 2019; 20: 1253-1258.
- Moreno-Egea A, Baena EG, Calle MC, Martínez JA, Albasini JL. Controversies in the current management of lumbar hernias. Arch Surg. 2007; 142: 82-8.
- Sharma P. Lumbar hernia. Med J Armed Force India. 2009; 65: 178-9.
- Hindawi, Case Reports in Surgery. 2020; 8859106.
- Radhakrishna V, et al. Int Surg J. International Surgery Journal. 2017; 4: 1472-1474.
- Aza et al. Journal of Medical Case Reports. 2023; 17: 145.
- Meinke AK. Totally extraperitoneal laparoendoscopic repair of lumbar hernia. Surg Endosc. 2003; 17: 734-7.
- Yusuf Sevim, et al. Grynfeltt Hernia with Spiegel Hernia: Report of a Rarely Encountered Case Running Head: Grynfeltt Hernia. ARC Journal of Surgery. 2017; 3: 1-4.