
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
A patient with refractory hyperlipidemia and hypothyroidism: A challenging final diagnosis
Christos Georgopoulos1; Matilda Florentin2*; Anila Duni1; Georgios Liapis3; Charalampos Milionis2; Evangelia Dounousi1
1Department of Nephrology, University Hospital of Ioannina, Ioannina, Greece
2Department of Internal Medicine, University Hospital of Ioannina, Ioannina, Greece.
3Department of Pathology Medical School, National and Kapodistrian University of Athens, Athens, Greece.
*Corresponding Author : Matilda Florentin
Department of Internal Medicine, University Hospital of Ioannina, Ioannina, Greece.
Email: matildaflorentin@yahoo.com
Received : Nov 13, 2023
Accepted : Dec 11, 2023
Published : Dec 18, 2023
Archived : www.jcimcr.org
Copyright : © Florentin M (2023).
Abstract
We present a case of a 47-year-old female patient with hyperlipidemia and hypothyroidism who was finally diagnosed with nephrotic syndrome. Specifically, the patient was referred and admitted to the Nephrology Department from her primary care physician who was investigating her for refractory hyperlipidemia; the patient was previously well controlled with lipid lowering treatment whereas hypothyroidism (as a secondary cause of hypercholesterolemia) was treated. Subsequently, the physician noted only mild edema of the lower extremities and proteinuria of nephrotic range. In this context, a serious condition, such as nephrotic syndrome did not go unnoticed.
Keywords: Edema; Hypercholesterolemia; Nephrotic syndrome.
Citation: Georgopoulos C, Florentin M, Duni A, Liapis G, Milionis C, et al. A patient with refractory hyperlipidemia and hypothyroidism: A challenging final diagnosis. J Clin Images Med Case Rep. 2023; 4(12): 2741.
Introduction
The typical clinical and laboratory features of a patient with nephrotic syndrome are those of nephrotic range proteinuria, low serum albumin and excessive edema, hyperlipidemia and lipiduria [1]. The differential diagnosis of this syndrome encompasses systemic diseases, such as diabetes mellitus and amyloidosis, as well as renal-limited entities such as membranous nephropathy, Minimal Change Disease (MCD), primary or secondary focal segmental glomerulosclerosis, membranoproliferative glomerulonephritis and deposition diseases [2,3].
Case presentation
A 47-year-old female patient was referred and admitted to the Nephrology Department for further evaluation of proteinuria. The patient was routinely evaluated by an Internal Medicine physician for hypercholesterolemia and hypothyroidism due to Hashimoto disease and she was well-controlled under treatment with L-thyroxine and rosuvastatin/ezetimibe combination. However, at a follow-up visit the laboratory exams revealed elevated levels of TSH (10.2 μIU/mL) and LDL-C (282 mg/ dl). The treating physician attributed hypercholesterolemia to the deregulation of the thyroid function and adapted the dose of L-thyroxine accordingly. A few weeks later, the laboratory exams demonstrated restoration of hypothyroidism (TSH=2.88 μIU/mL), while hypercholesterolemia still persisted. The patient consistently confirmed adherence to treatment and denied taking any other medication or over-the-counter dietary supplement, whereas her body weight was stable with a body mass index of 26 kg/m2 . She also had no symptoms or complaints. A thorough clinical examination revealed only mild bilateral symmetrical edema of the lower extremities
In this context, causes other than hypothyroidism for secondary hypercholesterolemia (Table 1) should be excluded.
The patient was not obese, had no cholestasis, diabetes or abnormal glucose metabolism parameters. Among other relevant laboratory examinations and taking into account the pitting edema of the lower extremities, the internist ordered a urine analysis. The latter was positive for 3+ proteinuria with no hematuria, pyuria or casts. Due to abnormal urine analysis along with hyperlipidemia deterioration, a 24-hour urine protein excretion was ordered, which revealed nephrotic range proteinuria of approximately 3.5 g of total protein. Therefore, the patient was admitted to the Nephrology Department for further evaluation.
On admission to the Nephrology Department the mild edema of the lower extremities was confirmed, while the rest clinical examination was insignificant. Complete blood count, liver enzymes, thyroid function and serum electrolytes were within normal limits. Her serum creatinine level was normal, and the estimated glomerular filtration rate (eGFR CKD-EPI) was calculated to 99 ml/min/1.73 m2 . Laboratory blood tests are depicted in Table 2. The kidney ultrasound revealed kidneys of normal size and parenchymal thickness with no obstruction.
A thorough workup for the diagnostic evaluation of nephrotic syndrome, as recommended (Table 3), was performed.
Serum electrophoresis and immunofixation did not reveal any paraproteins, while serum phosholipase A2 receptor antibodies (PLA2R Ab) were negative. Antinuclear antibodies, antineutrophil cytoplasmic antibodies (targeting myeloperodixase and proteinase-3) were negative and complement (C3, C4) levels were within normal limits. Evaluation for chronic infections, including Mantoux skin test and interferon Gamma release assay, hepatitis B, hepatitis C and HIV were negative as well, as were also the serological tests for toxoplasma, leishmania and brucella. Finally, age-appropriate screening for malignancy was performed with endoscopy of the upper and lower gastrointestinal tract and imaging studies with no abnormal findings.
Based on the high clinical suspicion for primary nephrotic syndrome and the negative serologic test for anti-PLA2R Ab, the patient underwent kidney biopsy which was compatible with diffuse podocytopathy. According to light microscopy examination, the sample included 24 glomeruli with only one showing global glomerular sclerosis (4%). The glomeruli were normal or with slightly increased size and there were no signs of focal segmental sclerosis in any glomeruli (Figure 1). No pathological findings were observed at the mesangium. Interstitial fibrosis and tubular atrophy score was calculated at 15-20%. No complement or immunoglobulin deposits were found at immunofluorescence microscopy. Electronic microscopy examination showed diffuse effacement of the epithelial foot processes.
A differential diagnosis guide of nephrotic syndrome based on histopathological findings is presented in Table 4.
Treatment
Based on clinical, laboratory and biopsy results, the patient’s diagnosis was MCD. According to current guidelines [4], the first line treatment in MCD includes corticosteroids. In our case, the patient was initiated on oral methylprednisolone at a dose of 64 mg once daily. The patient responded well to the corticosteroid treatment with complete remission achieved within two months after treatment initiation.
Table 1: Secondary causes of dyslipidemia.
| • Diabetes mellitus • Cholestatic liver disease • Nephrotic syndrome • Hypothyroidism • Obesity • Chronic Kidney Disease • Excessive alcohol consumption • Medications (beta-blockers, thiazide diuretics, oral estrogens, etc.) |
Table 2: Laboratory results of the patient and normal ranges*.
| • Urea: 22 mg/dl (75-125 mg/dl) • Creatinine: 0.75 mg/dl (0.6-1.2 mg/dl) • e-GFR: 99 ml/min/1.73 m2 • Albumin: 3.0 g/dl (3.4-5.0 g/dl) • Hemoglobin: 13.9 g/dl (12.0-15.0 g/dl) • WBC: 5640/μL (3800-11800/Μl) • ESR: 35 mm/h (0-30 mm/h) • Total Cholesterol: 350 mg/dl (110-200mg/dl) • Triglycerides: 220 mg/dl (40-175 mg/dl) • HDL-C: 42 mg/dl (35-70 mg/dl) • LDL-C: 264 mg/dl (60-130 mg/dl) • Non-HDL-C: 308 mg/dl • AST: 10 IU/L (10-35 IU/L) • ALT: 12 IU/L (10-35 IU/L) • HbA1c: 5,8% (4.3-6%) • CRP: 2 mg/L (<6 mg/L) • TSH: 2,88 mU/L (0.38-5.33 mU/L) • ΗbA1c=5.5% *normal ranges are shown in brackets |
WBC: White Blood Cells; PLT: Platelets; ESR: Erythrocyte Sedimen- tation Rate; CRP: C-Reactive Protein; eGFR: estimated Glomerular Fil- tration Rate (calculated by CKD-EPI formula); HbA1c: Hemoglobin A1c; TSH: Thyroid Stimulating Hormone; AST: Aspartate Aminotransferase; ALT: Alanine Aminotransferase; HDL-C: High Density Lipoprotein Cho- lesterol; LDL-C: Low Density Lipoprotein Cholesterol.
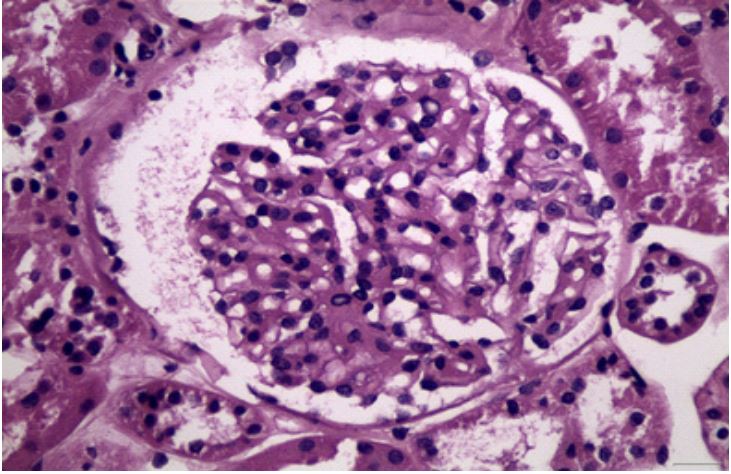
Table 3: Recommended diagnostic evaluation in patients with nephrotic syndrome.
| • Seek nephrology consultation • Thorough patient history • Laboratory testing Assess kidney function (urea/creatinine) Measure albumin Lipid panel Urine analysis with microscopy Confirm proteinuria with either 24h urine collection or random urine sample • Additional Laboratory testing HbA1c ANA, anti-dsDNA MPO-ANCA, PR3-ANCA C3, C4 HBV, HCV, and HIV tests Anti-PLA2R Ab Serum and urine electrophoresis/immunofixation Serum free light chains and immunofixation Evaluation for chronic infections (interferon Gamma release assay etc.) • Age-appropriate screening for malignancies • Perform a kidney biopsy |
HbA1c: Hemoglobin A1c; ANA: Anti-Nuclear Antibodies, anti-dsD- NA: Anti-double stranded DNA antibodies; MPO-ANCA: Antineutro- phil Cytoplasmic Antibodies Targeting Myeloperoxidase Protein; PR3- ANCA: Antineutrophil Cytoplasmic Antibodies Targeting Proteinase 3; HBV: Hepatitis B Virus; HCV: Hepatitis C Virus; HIV: Human Immunode- ficiency Virus; anti-PLA2R Ab: antiphospholipase A2 receptor antibod- ies.
Table 4: Histopathological Differential Diagnosis of nephrotic syndrome [5].
| • Membranous Nephropathy primary or secondary • Podocytopathies Primary MCD Primary FSGS Infections-HIV Drugs/toxins Malignancies, Hodgkin lymphoma urine sample • Membranoproliferative glomerulonephritis Systemic lupus C3 or C4 glomerulopathy Infections, HCV Malignancies • Deposition diseases Diabetes mellitus Amyloidosis Monoclonal deposition disease |
MCD: Minimal Change Disease; FSGS: Focal Segmental Glomerulo- sclerosis; HIV: Human Immunodeficiency Virus; HCV: Hepatitis C Virus.
Discussion
Nephrotic syndrome is a complex kidney disorder characterized by proteinuria, hypoalbuminemia, edema and hyperlipidemia. This syndrome frequently necessitates a multidimensional approach for its diagnosis, employing a combination of tests and examinations (Table 2). In every case diagnostic screening should be individualized, considering the patient’s age, gender, medical history, and specific risk factors [3]. Kidney biopsy remains the gold standard diagnostic examination, which is often necessary to determine the underlying cause of nephrotic syndrome.
Nephrotic syndrome is primarily a condition that falls within the clinical domain of nephrology. Nevertheless, initial assessment of patients with nephrotic syndrome is commonly made by primary or secondary care physicians [3]. Patients may complain of non-specific, varying symptoms which could mirror either the primary condition or one of its complications. Moreover, the fact that the prevalence of nephrotic syndrome is infrequent in non-nephrology clinical practice compared with chronic kidney disease and albuminuria due to diabetes and hypertension, frequently results in remarkable delayed or overlooked diagnosis. The typical clinical picture of full blown nephrotic syndrome is edema, the morning periorbital edema in the early stages which gradually worsens and appears on the legs, while if neglected, ascitic, pleural and pericardial effusions may also develop. In our case, patient at the time of assessment by the internist had only mild leg edema, that was actually asymptomatic and could easily go unnoticed by the physician as well. Importantly, the mild lower leg edema along with resistant to treatment hypercholesterolemia were noticed and were the early indications for reaching timely the final diagnosis of nephrotic syndrome, after considering all secondary causes of dyslipidemia.
Nephrotic syndrome is often associated with severe hyperlipidemia. Secondary hyperlipidemia accounts for almost 30-40% of all causes of hyperlipidemia. Differential diagnosis of secondary hyperlipidemia, as shown in Table 1, includes a remarkable number of divergent causes. It is of paramount importance to discriminate between these different pathogenetic entities before merely initiating lipid lowering therapy. In the case of our patient, the internist had to face an important yet uncommon diagnostic challenge; the fact that secondary hyperlipidemia was attributed to two distinct diseases, i.e. the already known hypothyroidism and the emerging nephrotic syndrome. Previously, the patient’s hypercholesterolemia and hypothyroidism were well controlled with rosuvastatin/ezetimibe combination and Lthyroxine accordingly. On this base, the internist, hierarchically and methodically adapted the dose of L-thyroxine in order to control thyroid hormones. When a few weeks later, the laboratory exams demonstrated resistant hypercholesterolemia, albeit restoration of hypothyroidism, the physician suspected the existence of a second cause of hyperlipidemia, although very rare in clinical practice. Subsequently, he proceeded with differential diagnosis. A 24-hour urine protein excretion was ordered, among other exams, which revealed nephrotic range proteinuria. Subsequently, the patient was immediately referred to a nephrologist allowing the early diagnosis of MN as the primary kidney disease of nephrotic syndrome.
As already mentioned, specialties other than nephrologists are usually the first to evaluate patients with symptoms and laboratory exams suggestive of nephrotic syndrome. The described case report, emphasizes the importance of good knowledge and familiarity of nephrotic syndrome by other medical specialists, in order to avoid delayed diagnosis and possible severe complications. Therefore, their role in recognizing the condition promptly, guiding further diagnostic tests and referring patients to nephrologists for further evaluation and management once the diagnosis of nephrotic syndrome is established, is crucial.
Declarations
Conflict of interest: None.
Patient consent: The patient signed an informed consent, offering us full permission to publish her data.
Author contributions: All authors contributed to the acquisition of data and writing of the case report. They all reviewed and edited the content.
References
- Wang C, Greenbaum LA. Nephrotic Syndrome. Pediatric Clinics of North America. 2019; 66: 73-85.
- Kopp JB, Anders HJ, Susztak K, Podestà MA, Remuzzi G, et al. Podocytopathies. Nature Reviews Disease Primers. 2020; 6: 68.
- Politano SA, Colbert GB, Hamiduzzaman N. Nephrotic Syndrome. Primary Care: Clinics in Office Practice. 2020; 47: 597-613.
- Rovin BH, Adler SG, Barratt J, Bridoux F, Burdge KA, et al. KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney International. 2021; 100: S1-S276.
- O’Shaughnessy MM, Hogan SL, Thompson BD, Coppo R, Fogo AB, et al. Glomerular disease frequencies by race, sex and region: Results from the International Kidney Biopsy Survey. Nephrology Dialysis Transplantation. 2018; 33: 661-669