
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Stone formation caused by hem-o-lok clip migration into common bile duct after laparoscopic cholecystectomy and choledocholithotomy: A case report
Haidong Zhang1*; Xian Su1*; Cunzhen Zhang2*; Nan Li2†; Minfeng Zhang1†; Haibei Xin1†
1Department of Hepatobiliary Surgery, Shanghai Municipal Hospital of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, China.
2Department of Hepatic Surgery I (Ward I), The Third Affiliated Hospital of Naval Military Medical University, Shanghai, China.
†Contributed equally to this work.
*Corresponding Author : Haidong Zhang, Xian Su
Department of Hepatobiliary Surgery, Shanghai
Municipal Hospital of Traditional Chinese Medicine,
Shanghai University of Traditional Chinese Medicine, Shanghai, China.
Email: seu_hz@163.com; suxian9504@163.com
*Corresponding Author : Cunzhen Zhang
Department of Hepatic Surgery I (Ward I), The Third
Affiliated Hospital of Naval Military Medical University, Shanghai, China.
Email: zhangcunzhenzcz@126.com
Received : Nov 14, 2023
Accepted : Dec 12, 2023
Published : Dec 19, 2023
Archived : www.jcimcr.org
Copyright : © Zhang H, Su X, Zhang C (2023).
Abstract
Background: Stone formation due to the migration of hem-o-lok clip into the common bile duct after laparoscopic surgeries remains rare. Here, we reported a case of acute cholangiolithiasis caused by hem-o-lok clip migration into the common bile duct 3 years later after laparoscopic surgeries.
Case presentation: A 44-year-old woman characterized by right upper quadrant pain for one week. The patient had received laparoscopic cholecystectomy and choledocholithotomy with T-tube drainage to deal with cholecystolithiasis and choledocholithiasis 3 years previously. Two hem-o-lok clips were left in the stumps of the cystic duct and the cystic artery after the surgery. Diagnosis of multiple stones in intrahepatic and extrahepatic bile duct was confirmed by MRCP. The patient was successfully cured by laparotomy with T-tube drainage to remove the stone and clip in common bile duct and was discharged from hospital after one week.
Conclusions: Although rare, clip migration with biliary complications needs to be considered in the differential diagnosis of patients presenting with post-cholecystectomy problems. Moreover, hem-o-lok clip should be carefully used during laparoscopic surgery and the Hemo-lok clip should not be in close proximity to the incision on common bile duct.
Keywords: Hem-o-lok clip; Migration; Common bile duct; Laparoscopic surgery; Cholangiolithiasis.
Abbreviations: NR: Normal range; CT: Computed tomography; MRCP: Magnetic resonance cholangiopancreatography.
Citation: Zhang H, Su X, Zhang C, Li N, Zhang M, et al. Stone formation caused by hem-o-lok clip migration into common bile duct after laparoscopic cholecystectomy and choledocholithotomy: A case report. J Clin Images Med Case Rep. 2023; 4(12): 2742.
Background
Approximately 10% to 15% of the adult population suffers from gallstone disease and cholelithiasis [1]. Laparoscopic cholecystectomy and choledocholithotomy with stone removal is common and preferred for gallstone disease treatment, while surgical common bile duct exploration is considered as the final option [2]. Moreover, these two methods are also common surgical procedures for postoperative recurrence of cholelithiasis. The Hem-o-lok clip is widely used in laparoscopic surgeries of various disciplines, including the urinary system, hepatobiliary system and gastrointestinal system. The hem-o-lok clip is easy to use and helpful for shortening the operation time and lowering the rate of converting to open surgery [3,4]. However, there is a risk that the placed clip can migrate into the common bile duct post-operation, leading to hemorrhage and bile leakage, or recurrence of stones. The mechanism of clip migration is poorly understood. It may be a complex process involving ineffective clip placement, inflammation around the biliary tract with localized necrosis, and pressure exerted from intra-abdominal organ movement [5]. The exact incidence is also unknown. Fewer than 75 cases have been reported in the English literature. We report a case of hem-o-lok clip migration into the common bile duct with stone formation 3 years after laparoscopic surgeries. The patient was successfully treated by laparotomy with T-tube drainage to remove the stone and clip in common bile duct.
Case presentation
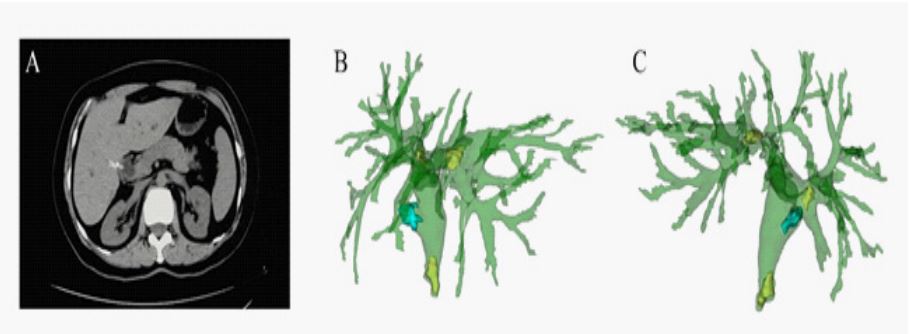
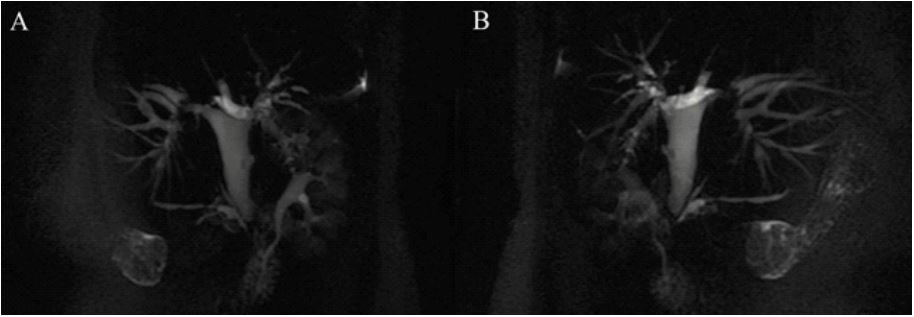
A 44-year-old woman presented with recurrent right upper quadrant pain for 1 week. She had received laparoscopic cholecystectomy and choledocholithotomy with T-tube drainage to deal with cholecystolithiasis and choledocholithiasis in June 2018 in local hospital. Two hem-o-lok clips were used to occlude the cystic duct and cystic artery before removal of the gall bladder. A T-tube was placed after the removal of common bile duct stones and was pulled out 3 months later. Then the woman was admitted to our hospital for the recurrence of gallstones in June 2021. Physical examination showed abdominal tenderness, and laboratory testing revealed the following routine blood parameters: White blood cell count of 3.82×109/L (normal range [NR]: 3.5-9.5×109 /L) and neutrophil percentage of 0.62 (NR: 0.5-0.7). Liver function parameters were as follows: total bilirubin of 11.6 mmol/L (NR: 6.8-30 mmol/L), alanine aminotransferase of 17 U/L (NR: 9-50 U/L), aspartate aminotransferase of 57 U/L (NR: 15-40 U/L). Ultrasound showed that the inner diameter of common bile duct was 15 mm, the inner diameter of right hepatic duct is 7 mm and the inner diameter of left hepatic duct is 6 mm, followed by specific strong echoes in right hepatic lobe (Figure 1). Three-dimensional CT (Figure 2) and MRCP (Figure 3) identified multiple stones formation in left intrahepatic bile duct and extrahepatic bile duct with the stenosis of distal common bile duct and intrahepatic bile duct in right hepatic lobe and caudate lobe. Then common bile duct incision and exploration, intrahepatic and extrahepatic bile duct stone removal and T-tube drainage were performed. Intraoperative exploration revealed the heavy adhesion of gall bladder bed and omentum majus. The common bile duct was thickened with a diameter of 15 mm. A 10 mm stone in the lower common bile duct and an 8 mm stone near the opening of middle gallbladder duct were detected after the longitudinal incision of upper common bile duct. Further, a white hem-o-lok clip was exposed after the removal of stones with one end fixed in the bile duct (Figure 4). The hem-o-lok clip was cut and removed completely. The left and right hepatic ducts were expanded and several stones were removed. A T-tube of 24F was left in the right hepatic duct and common bile duct. Finally, the patient was discharged smoothly one week later after liver protection and anti-inflammatory treatments.


Discussion
Hem-o-lok clip migration into common bile duct is a rare but well-recognised complication of laparoscopic surgeries. It was first noted in 1979 after open cholecystectomy [6], and in 1992 after laparoscopic cholecystectomy [7]. More than 100 cases of hem-o-lok clip migration after laparoscopic surgeries were reported until now [8]. Clips migration into the bile duct may function as a nidus for the gallstone formation causing biliary obstruction.
The mechanism responsible for hem-o-lok clip migration remains speculative. Some possible hypotheses of pathogenesis were suggested. Raoul suggested that surgical clips which were applied improperly and incomplete closure of cystic duct would allow development of biloma, which could be drained off later into the common bile duct through the cystic duct [7]. Others hypothesised that localized inflammatory process may lead to erosion of the bile duct wall, which results in the surgical clip migrating into the ductal system. Kitamura presented that the surrounding structures pressed the clipped cystic duct, which then becomes inverted into the lumen of the common bile duct [9]. Also, an inflammatory-rejection response to the surgical clip as a foreign body is also a possibility [10]. In severe acute cholecystitis, it is difficult to accurately place the clip in the exact position because of the deformity of the anatomical structures, which was caused by severe inflammation and adhesions [11]. In the present case, stones and a hem-o-lok clip were found near the opening of middle gallbladder duct during the laparotomy. A possible explanation for hem-o-lok clip migration may be that the cystic duct ligation site was close to the incision on the common bile duct and a rejection response led to this migration, and then it gradually migrated into the common bile duct.
The time interval for hem-o-lok clip migrating into the bile duct after laparoscopic surgeries varies from 11 day to 20 years [12]. The representative symptoms, including abdominal pain, fever, jaundice due to biliary obstruction and sepsis due to ascending cholangitis, are not different from those of non-iatrogenic choledocholithiasis. The diagnosis can be made based on the noninvasive imaging, such as X-ray, ultrasound, Computed Tomography (CT) and Magnetic Resonance Cholangiopancreatography (MRCP) [13]. In the present case, preliminary diagnosis was made on the basis of abdominal ultrasound and CT scan, and final diagnosis was confirmed by laparotomy. Management of this complication is straightforward. Endoscopic retrograde cholangiography with sphincterotomy and stone as well as clip removal should be the main modality of choice. Laparotomy or percutaneous transhepatic cholangiography remains as the rescue procedures, especially in the presence of difficult biliary stricture or large stones [14]. Lastly, every effort should be made to prevent this complication by addressing the contributory factors.
The type of surgical clip may also influence the occurrence of clip migration. Hem-o-lok clip, which was applied in this case, is a non-absorbable polymer clip generally used to ligate cystic duct. In some studies, application of absorbable clips lowered the risk of migration compared with non-absorbable clips. However, Cetta suggested that absorbable clips could also cause clip migration and be a nidus of stone formation [15]. According to recent literatures, clipless cholecystectomy using a harmonic scalpel may be a safer alternative option for avoiding complications [16]. Harmonic scalpel was accepted as a reasonable alternative for closure of cystic duct and has provided shorter operation time and fewer complications of bile leaks and gallbladder perforation [17]. However, absorbable suture or harmonic scalpel are not used routinely due to the high cost of their applications.
Conclusion
Although rare, clip migration with biliary complications needs to be considered in the differential diagnosis of patients presenting with postcholecystectomy problems. Thereby, timely improvement of relevant examinations is required for differential diagnosis and subsequent treatment. Moreover, a hem-o-lok clip should be carefully used during laparoscopic surgeries, which should not be too close to the incision on the common bile duct.
Declarations
Acknowledgments: The authors are grateful to the patient, researchers, and institutions that participated in the present study.
Funding: Not applicable
Availability of data and materials: The original data for this case is obtained from the third Affiliated Hospital of Naval Military Medical University. More specific data used in this study are available from the authors upon reasonable request and with permission of the third Affiliated Hospital of Naval Military Medical University.
Ethics approval and consent to participate: All data in this article have been approved by the patient and the third Affiliated Hospital of Naval Military Medical University. This study was in line with the 1964 Helsinki Declaration and subsequent amendments or similar ethical standards.
Competing interests: All authors declare that they have no competing interests.
Consent for publication: Not applicable
Authors’ contributions: HDZ and HBX discovered the particularity of the case and collected the relevant information. HDZ, XS, CZZ completed the manuscript. NL and MFZ improved the figures. HDZ and XS completed the manuscript. NL, MFZ, HBX proofread the manuscript. All authors contributed to the article and approved the submitted version.
References
- Buturovic S. Iatrogenic injury to the common bile duct. Med Arch. 2014; 68: 291-3.
- Hassler KR, Collins JT, Philip K, Jones MW. Laparoscopic Cholecystectomy. Treasure Island (FL). 2021.
- Turini GA 3rd, Brito JM 3rd, Leone AR, et al. Intravesical Hemostatic Clip Migration after Robotic Prostatectomy: Case Series and Review of the Literature. J Laparoendosc Adv Surg Tech A. 2016; 26: 710-2.
- Hamamoto S, AbdelRazek M, Naiki T, et al. LigaSure versus the standard technique (Hem-o-lok clips) for robot-assisted radical prostatectomy: A propensity score-matched study. J Robot Surg. 2021.
- García Reyes A, López-Cantarero García-Cervantes M, Bellido Luque JA, Sánchez-Matamoros Martín I, Nogales MÁ. Clip migration after cholecistectomy. Rev Esp Enferm Dig. 2021.
- Rou WS, Joo JS, Kang SH, et al. Abdominal Pain Due to Hem-olok Clip Migration after Laparoscopic Cholecystectomy. Korean J Gastroenterol. 2018; 72: 313-317.
- Raoul JL, Bretagne JF, Siproudhis L, Heresbach D, Campion JP, et al. Cystic duct clip migration into the common bile duct: A complication of laparoscopic cholecystectomy treated by endoscopic biliary sphincterotomy. Gastrointest Endosc. 1992; 38: 608-11.
- Ito T, Shimatani M, Masuda M, et al. Endoscopic retrieval of a migrated surgical clip in a choledochojejunal anastomosis using the rendezvous technique. Endoscopy. 2021.
- Kitamura K, Yamaguchi T, Nakatani H, et al. Why do cystic duct clips migrate into the common bile duct. Lancet. 1995; 346: 965-6.
- Minamida S, Iwamura M, Soh S, et al. Spontaneous migration of a metal clip into renal pelvis after laparoscopic pyeloplasty: A case report. Nihon Hinyokika Gakkai Zasshi. 2007; 98: 835-8.
- Panara A, Barkin JA, Barkin JS. Postcholecystectomy Biliary Clip Migration Causing Acute Pancreatitis. ACG Case Rep J. 2019; 6: e00221.
- Chen GH, Zhu TM, Xu XL, Jiang KX. Migration of metal clips into the duodenum after laparoscopic cholecystectomy: A report of two cases. J Int Med Res. 2018; 46: 2458-2460.
- Roh YJ, Kim JW, Jeon TJ, Park JY. Common bile duct stone development due to a Hem-o-lok clip migration: A rare complication of laparoscopic cholecystectomy. BMJ Case Rep. 2019; 12.
- Angelescu M, Enciu O, Florescu V, Miron A. Obstructive Jaundice Secondary to Clip Migration in the Common Bile Duct 9 Years after Laparoscopic Cholecystectomy. Chirurgia (Bucur). 2020; 115: 526-529.
- Cetta F, Baldi C, Lombardo F, Monti L, Stefani P, et al. Migration of metallic clips used during laparoscopic cholecystectomy and formation of gallstones around them: Surgical implications from a prospective study. J Laparoendosc Adv Surg Tech A. 1997; 7: 37-46.
- Liao G, Wen S, Xie X, Wu Q. Harmonic Scalpel versus Monopolar Electrocauterization in Cholecystectomy. JSLS. 2016; 20.
- Rajnish K, Sureshkumar S, Ali MS, Vijayakumar C, Sudharsanan S, et al. Harmonic Scalpel-Assisted Laparoscopic Cholecystectomy vs. Conventional Laparoscopic Cholecystectomy - A Nonrandomized Control Trial. Cureus. 2018; 10: e2084.