
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
A case with community-acquired pneumonia caused by nocardia
Tuba Ciftci1; Adem Dirican1; Sara Tarek Bin Zabyah2; Doga Ozkaya3; Sevket Ozkaya1*
1Department of Pulmonary Medicine, Faculty of Medicine, Altinbas University, Istanbul, Turkey.
2Medical Student, Faculty of Medicine, Altinbas University, Istanbul, Turkey.
3Medical Student, Faculty of Medicine, Palacky University, Olomuc, Czech Republic.
*Corresponding Author : Sevket Ozkaya
Professor in Medicine, Department of Pulmonary
Medicine, Faculty of Medicine, Altinbas University,
Istanbul, Turkey.
Tel: +90-532-4741309;
Email: ozkayasevket@yahoo.com
Received : Nov 13, 2023
Accepted : Dec 12, 2023
Published : Dec 19, 2023
Archived : www.jcimcr.org
Copyright : © Ozkaya S (2023).
Abstract
Nocardiosis is a disease affecting different organs of the body and pulmonary forms of nocardiosis are induced via aerosolized inoculation of the bacterium into the airways. The infection causes pneumonia-like symptoms. Pulmonary nocardiosis clinically appears similar to many other viral, bacterial, or fungal infections as well as several types of malignancy and tuberculosis.
We aimed to discuss a case with Pulmonary Nocardiosis presented as community-acquired pneumonia.
Keywords: Nocardia; Pulmonary nocardiosis; Community-acquired pneumonia.
Citation: Ciftci T, Dirican A, Bin Zabyah ST, Ozkaya D, Ozkaya S. A case with community-acquired pneumonia caused by nocardia. J Clin Images Med Case Rep. 2023; 4(12): 2743.
Introduction
Worldwide, the aerobic actinomyces genus Nocardia is found in both freshwater and saltwater habitats, as well as a range of soil types. A nocardia is a branching, filamentous, gram-positive organism having mildly positive characteristics for acid fastness. Nocardia infection is an uncommon bacterial illness that typically affects the skin, brain, and lungs [1,2]. Rare and opportunistic, nocardia is a very rare form of CommunityAcquired Pneumonia (CAP) that mostly affects patients with a compromised immune system. We report a Nocardia-caused pneumonia case that was reported by CAP.
Case presentation
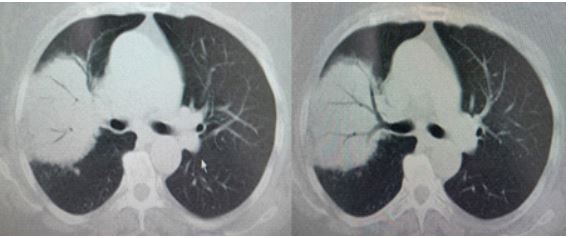
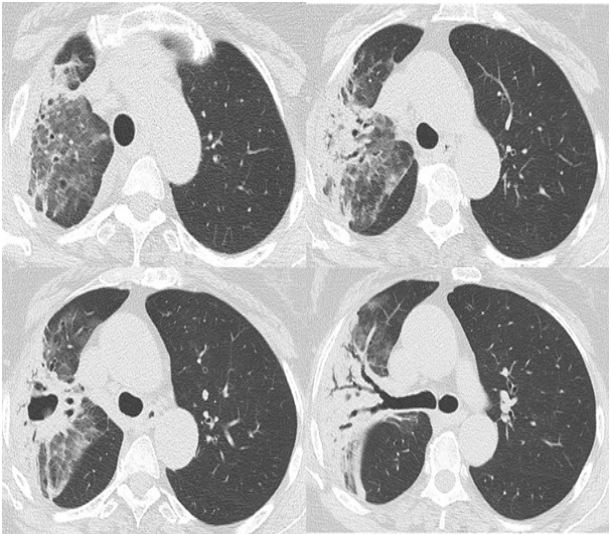
A 50-year-old female nonsmoker was admitted to the outpatient clinic complaining of fever, coughing, and dyspnea that had been present for ten days. Her diabetes mellitus and hypertension were well controlled by the use of olmesartan and metformin. A physical examination found a temperature of 38.9 degrees Celsius as well as coarse crackles. The alveolar infiltration with air-bronchograms in the right upper lobes was detected on thoracic CT scans (Figure 1).
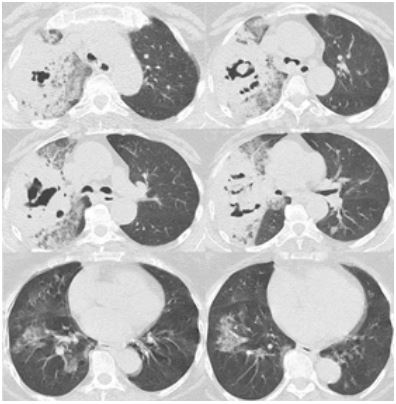
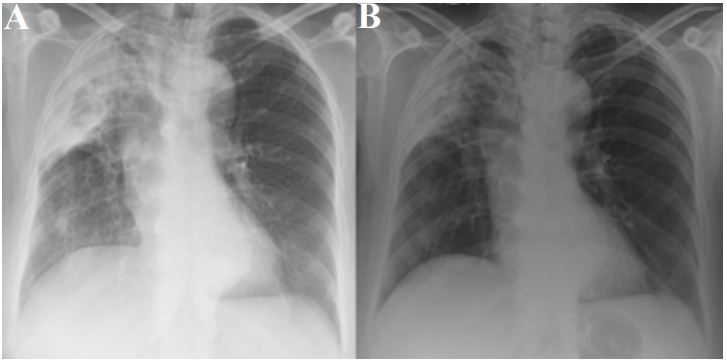
The results of the laboratory were as follows: sedimentation rate of 79 mm/h; BUN of 52.6 mg/dL; creatinine of 2.3 mg/dL; and Na of 126 mEq/L. Negative for ANA, p-ANCA, c-ANCA, and anti-CCP. It was intended to receive pneumonia treatment while in the hospital. Treatments with levofloxacin and piperacillin/ tazobactam were initiated. Despite receiving treatment for ten days, no progress has been observed in the clinic or radiologically. She was referred to our clinic due to respiratory failure and pneumonia that were not improving with medication. Chest roentgenography revealed the bilateral opacities and a necrotic alveolar opacity that completely covered the right upper lobe (Figure 2A). A second thoracic CT scan was performed. Bilateral infiltrations with thick-walled cavitary and necrotic alveolar opacities occurred (Figure 2B).
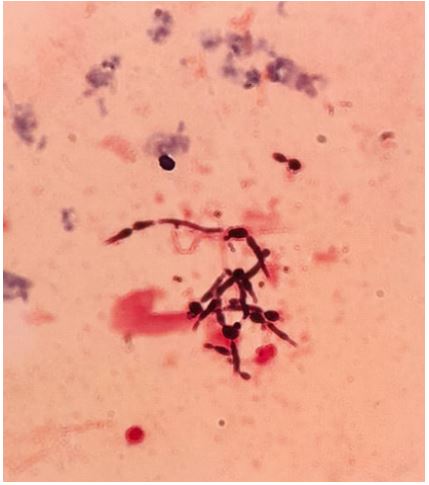
Examination of the sputum smear revealed no tubercle bacilli. We considered that either actinomyces or nocardia might be the cause of these radiologic and clinical findings. We used Gram staining for the sputum smear. The organisms identified by the sputum smear were Gram-positive rods with branching chains that resembled fungal hyphae, which was consistent with a typical Nocardia colony (Figure 3).
We started the trimethoprim/sulfamethoxazole (TMP/SMX) treatment for pulmonary nocardiosis-pneumonia, and she rapidly clinically and radiologically responded to treatment. She was discharged after 15 days of treatment (Figure 4A and 4B).

Discussion
Nocardia are ubiquitous saprophytes that can be found in soil, water, and decomposed organic waste. Bacteria can cause an uncommon disease called nocardia infection. Initially, nocardia presents as an opportunistic infection in immunocompromised hosts. It can affect nearly every part of the human body, such as the pleural or pulmonary system, the skin and its structures, or it can spread to other organ systems. Pulmonary forms of nocardiosis are induced via aerosolized inoculation of the bacterium into the airways. Dissemination across the rest of the body may occur from either of these initial inoculations. Pulmonary nocardiosis has a chronic course and a varied and nonspecific clinical presentation. When symptoms initially appear, they typically last for several days or weeks. In this case, the symptoms existed for a period of two weeks prior to being referred to our medical facility. Fever, a productive cough, and dyspnea are the main symptoms. In this case, a low-grade fever, weakness, and a persistent cough with productive sputum were the presenting symptoms. Pleomorphic and nonspecific radiographic manifestations are seen in the chest. The most frequent abnormalities are consolidations and large irregular nodules, which are frequently cavitary; interstitial patterns, masses, and nodules may also occur. More often affected are the upper .The results of computed tomography show many distinct lung nodules, pleural effusion, consolidation with or without cavitation, and chest wall extension [1-6].
CT chest and plain film chest radiography should be used in imaging investigations to evaluate for pulmonary infections. Radiography may reveal irregular nodules, cavitation, widespread alveolar pulmonary infiltrates, lung abscess, or pleural effusion, even though there are no classical manifestations [3].
Considering the nonspecific nature of the clinical and radiologic presentations and the challenges associated with microbiological identification, it is likely that pulmonary nocardiosis may be misdiagnosed in some individuals as diseases such as tuberculosis, bacterial pneumonia, or malignancy [4]. Sputum smears and ANCA profiles were examined in our instance in order to make a differential diagnosis. They were all in the negative.
Pulmonary nocardiosis can present as acute, subacute, or chronic infections. In addition, a clinical diagnosis of pneumonia or an inflammatory bronchial mass with a fever, productive cough, dyspnea, or chest pain is determined. As was the case with our patient, pulmonary disease can be made more complicated by cavitation, the development of an abscess, pleural effusion, or empyema. Under a microscope, Nocardia’s characteristic filamentous, beaded, and branching appearance is clearly visible. Furthermore, a diagnosis cannot be made if the doctor has no suspicions about nocardia. Seven species have been associated with human disease. Approximately 70% of infections produced by these organisms are caused by Nocardia asteroids, which, even with appropriate therapy, have a 45% fatality rate in debilitated patients. There are very few reports of cases about Nocardia treatment outcomes. Individuals who are immune-compliant or who have received a transplant have a more uncertain outlook than individuals who have an intact immune system. If excessive morbidity and mortality are to be avoided, an interdisciplinary approach to transplant patient care is necessary. The initial course of treatment for nocardiosis with antibiotics should continue for at least six months, and the treatment should be continued for at least one month after the infection’s symptoms have subsided. Skin infections in immunocompetent patients may be treated with monotherapy. Two to three medications should be part of an empirical therapy plan for pulmonary or disseminated disease. No therapy has yet been proven to be more successful than the others. As a result, antibiotic regimens should be customized according to culture and sensitivity patterns. Potential agents to use include trimethoprim/sulfamethoxazole, amikacin, imipenem, meropenem, third-generation cephalosporins such as ceftriaxone and cefotaxime, minocycline, extended-spectrum fluoroquinolones such as moxifloxacin, linezolid, tigecycline, dapsone, and clarithromycin. First-line treatments are sulfonamides, particularly sulfadiazine, because of its high brain penetration. Trimethoprim-sulfamethoxazole is also preferred by some clinicians. Combination medication therapy is suggested for severe diseases [1-6].
We started the Trimethoprim/Sulfamethoxazole treatment for nocardia pneumonia, and she rapidly clinically and radiologically responded to treatment. After 3 weeks of treatment, pulmonary lesions were regressed, as seen in Figures 4A and 4B. She is currently undergoing treatment and follow-up, and we will provide updates on the long-term outcomes of her treatment.
Pulmonary Nocardiosis should be kept in mind in patient with CAP especially in non-responding to antibiotics.
Authors contributions: TC and DO contributed to the design and implementation of the research, to the analysis of the results and to the writing of the manuscript. SO and AD contributed to the patient care. STBZ contributed to the design of figures.
References
- Rawat D, et al. Nocardiosis, in StatPearls. Treasure Island (FL). 2023.
- Kumar AA, et al. Pulmonary nocardiosis: Under-diagnosed respiratory opportunistic infection-A case report. Radiology of Infectious Diseases. 2017; 4: 175-178.
- Jeffrey P Kanne, Donald R Yandow, Tan-Lucien H Mohammed, Cristopher A Meyer. CT Findings of Pulmonary Nocardiosis. American Journal of Roentgenology. 2011; 197: W266-W272.
- Aggarwal D, Garg K, Chander J, Saini V, Janmeja AK. Pulmonary nocardiosis revisited: A case series. Lung India. 2015; 32: 165-8.
- Mazzaferri F, et al. Nocardia infection over 5 years (2011-2015) in an Italian tertiary care hospital. New Microbiol. 2018; 41: 136- 140.
- Wilson JW. Nocardiosis: Updates and clinical overview. Mayo Clin Proc. 2012; 87: 403-7.