
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Extensor tendons rupture in rheumatoid wrist: The management challenge in the light of a clinical observation
Mariam Erraoui1,2*; Siham Rachidi1 ; Kamal Rafiqi3 ; Mohammed Amine Mahdi4 ; Imad Ghozlani2,5; Jihad Moulay Berkchi6
1Department of Rheumatology, Souss Massa University Hospital Center, Morocco.
2Carbone Research Team, LARISS Laboratory, Faculty of Medicine and Pharmacy of Agadir, Ibn Zohr University, Morocco.
3Department of Traumato-Orthopedics, Souss Massa University Hospital Center, Morocco.
4Rheumatologist, Liberal Sector Rabat-Salé, Morocco.
5Department of Rheumatology, Oued Eddahab Military Hospital, Agadir-Morocco.
6Department of Rheumatology, Cheikh Khalifa International University Hospital, Mohammed VI University of Health Sciences (UM6SS), Casablanca, Morocco.
*Corresponding Author : Mariam Erraoui
Department of Rheumatology, Souss Massa university Hospital Center, Morocco.
Email: mariama_erraoui@yahoo.fr
Received : Nov 14, 2023
Accepted : Dec 15, 2023
Published : Dec 22, 2023
Archived : www.jcimcr.org
Copyright : © Erraoui M (2023).
Abstract
Rheumatoid arthritis is a frequent inflammatory rheumatic disease. It is characterized by synovitis and tenosynovitis. Involvement of wrist is very common especially dorsal face in relation to extensor tendon tenosynovitis. Rupture of these tendon can be occurred as a complication in severe and active rheumatoid arthritis. In this review by projecting a case report, we describe extensor tendon injuries, risk factors for rupture and management of tendon rupture in rheumatoid hand.
Keywords: Rheumatoid wrist; Extensor tendon; Rupture.
Citation: Erraoui M, Rachidi S, Rafiqi K, Amine Mahdi M, Ghozlani I, et al. Extensor tendons rupture in rheumatoid wrist: The management challenge in the light of a clinical observation. J Clin Images Med Case Rep. 2023; 4(12): 2752.
Introduction
Rheumatoid arthritis is a frequent rheumatic disease characterized by synovitis and tenosynovitis which are frequent in the hand and the wrist. The involvement of the dorsal compartment of the wrist is most common. It is generally related to extensor tenosynovitis. In the presence of several risk factors, the evolution of these tenosynovitis can be a tendon rupture. Rupture of the long extensor tendons to the fingers is a common complication of rheumatoid arthritis, described the first time in 1948 by Vaughan-Jacksonfirst [1]. The incidence of an extensor tendon rupture at the wrist is about 4% and the prevalence of an additional rupture of another tendon is over 50%. Patients tolerate and compensate for long term extensor tendon ruptures leading to late clinical presentation [2]. Clinically, the diagnosis of rupture is not always evident. Tendon rupture may go unnoticed, it should be suspected if simple decrease in extension especially on the fifth finger. Ultrasonography (US) can be useful to detect abnormalities in tendons that can predict ruptures.
The management of rheumatoid hand is one of the challenging conditions for rheumatologists. Ideally, medical treatment should be effective in preventing structural damage and avoiding complications. But, if complications, such as tendon rupture, are installed, the surgical treatment can also be indicated. Surgical management is also delicate for orthopedists, especially if the destruction and deformities are already there.
In this paper, by exposing a clinical observation of extensor tendons rupture, we will focus on the injuries of the extensor tendons in rheumatoid arthritis, especially the Extensor Digiti Minimi (EDM) and the Extensor Digitorum Communis (EDC). Risk factors of ruptures and their challenging management are also detailed.
Case report
We report a case of 44-year-old women, right-handed with a diagnosis of rheumatoid arthritis associated with Gougerot Sjogren’s syndrome. She had a long history of arthralgia and dry eyes since 2012, but the diagnosis does not establish until 2016. In the management of her disease, she had received corticosteroid, methotrexate and hydroxychloroquine but she didn’t have a remission. She had a positive rheumatoid factor and sialadenitis with score 4. She always has dorsal swilling of the right wrist despite treatment. Radiographs objective destruction of carpe and scallop sign and bilateral diastasis of the inferior radioulnar joint (Figure 1). Ultrasonography objective tenosynovitis of extensor digitorum comminis (Figure 2), the extensor digiti minimi and also the extensor carpi ulnaris. She had also synovitis of the distal radio-ulnar joint. Tree month before her readmission in our department, she received a glucosteroid infiltration of tenosynovitis and she had a diminution of swelling and pain the two months after. In our examination, in addition to the wrist tumefaction still present, she had a loss of the extension of the 3rd, 4th and 5th fingers of the right hand (Figure 3). In ultrasonography, we found tenosynovitis of the extensor digitorum comminis and the extensor carpi ulnaris. Also, synovitis of distal radio ulnar joint was persistent. In transverse section of the fifth compartment, we had an empty synovial sheath (Figure 2). We referred the patient to surgery. Intraoperative exploration had shown significant tenosynovitis with rupture of the extensor tendons of the 3rd, 4th and 5th finger in zone 7 (Figure 3). This is associated with a loss of tendon substance of 3 cm. Graft from the extensor of the index finger was performed. Then a transfer of the 4th and 5th tendons on the tendons of the index and middle finger were done. Evolution after two months was favorable with reprise of extension (Figure 3).
Anatomical focus
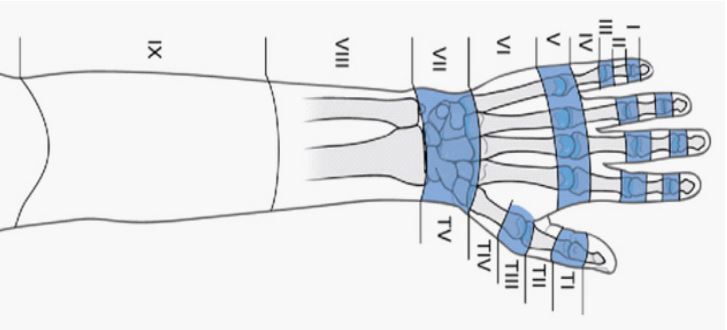
As its name suggests, the extensor apparatus of the hand ensures the extension of the fingers and the wrist. Muscles in forearm, called extrinsic muscles and innervated by the radial nerves, are extended by tendons crossing the dorsum of the wrist. These tendons in the wrist are arranged in 6 compartments delimited by 4 bony reliefs which are from medial to lateral: the radial crest, the Lister tubercle, the distal radio-ulnar joint and ulnar gutter. These compartments are anatomical tunnels which are arranged mainly on the dorsal face of the wrist, but also on the radial and ulnar faces. Before reaching the fingers, the extensor tendons pass under the retinaculum in the wrist. The extensor tendons are extra synovial except at the level of retinaculum where are surrounded by a synovial sheath which allows its lubrication and nutrition (Figure 4)[3].
The 1st compartment in the radial edge of the wrist includes the adductor policis longus and extensor policis brevis tendon. The 2nd compartment includes tenons of extensor carpi radialis longus and brevis. It is found within the anatomical snuff box, just ulnar of the radial styloid. In the 3rd, the extensor policis longus rests on Lister’s tubercle which serves as a pulley at this level. In the 4th compartment, we find the extensor digitorum communis in addition to the extensor indicis poprius, which is sometimes more difficult to identify on ultrasound examination. In the fifth compartment, the extensor digiti minimi is located on the palmar surface of the ulna, just medial of the distal radio-ulnar joint. Finally, the extensor carpi ulnaris occupy the 6th compartment alone (Figure 5).
This apparatus has some varieties especially in extensor indicis and extensor of the fifth finger. In 14% of cases we find a duplicated proper extensor of indicis. In 19% of cases, anatomical variations of the two tendons, proper and communis, at the metacarpal head are noted. On the fifth finger, the extensor digiti minimi, constant, consists of two tendons in 80% of cases. Sometimes, the common extensor of the fifth finger can be absent in 1 to 6% of cases depending on the series [4]. In surgical anatomy, injuries of extensor tendons such as rupture are defined by zones (Figure 6) [5]. In rheumatoid arthritis, most extensor tendons rupture occurs in the seventh zone.
Tendons injuries in rheumatoid hand
In rheumatoid arthritis, apart from joint damage, there is frequent tendon injuries. It is frequently a tenosynovitis which is predominantly located in dorsum of wrist [6]. In this location, the most frequent lesions interest the extensor digitorum communis and the extensor carpi ulnaris [7]. Clinically, tenosynovitis is suspected if presence of cystic swelling in the dorsum of the wrist. Ultrasonography confirm the diagnosis. It shows the presence of tenosynovitis like an “hypoechoic/anechoic thickened tissue with or without fluid within the tendon sheath, seen in two perpendicular planes and which may exhibit Doppler signal” as it is defined, by The OMERACT (Outcome Measures in Rheumatoid Arthritis Clinical Trials) group [8]. In rheumatoid arthritis, ultrasonography search also tendon damage, defined as the presence of tendon echotexture derangement, partial or complete tear. Rupture can be diagnosed if in US there is a complete loss of tendon substance visualized with the US beam exactly perpendicular to the tendon [9]. Most frequently, echotexture derangement and change of extensor tendons is present in the ECU tendon and the two tendons of the first compartment of extensor tendons [10,11]. The presence of inflammatory tenosynovitis of extensor carpi ulnaris, especially if ultrasonography shows a positive doppler, is predictive of structural progression [10,12]. Also, chronic inflammation of synovial sheath can lead to tendon rupture. The rupture is very evident if the patient has total loss of fingers extension. But, in some situations, it is not clinically apparent, especially if peritendinous synovia causes adhesion of the tendon ends and then the patient keep a certain degree of extension [2]. Isolated EDM rupture produces little functional loss and is often unnoticed because of the presence of EDC tendon to the fifth finger. When suspected, the diagnosis can be confirmed by firstly asking the patient to make a fist, to defunction the Extensor Digitorum Communis (EDC), and then to extend the little finger in isolation. If EDM is ruptured, there will be a lag of approximately 40 degree [13]. Multiple ruptures cause impaired function of several fingers and patients has markedly limitation of the hand’s grip strength [14].
Pathogenesis
In established rheumatoid arthritis the diagnosis is evident, especially if typical hand deformities are installed. These deformities can lead from different origins. Carpe erosion and destruction associated with mectacarpo-phalangial dislocation or subluxation associated with synovitis and tenosynovitis in the wrist are the major causes of hand disorganization [15,16]. The pathogenesis of extensor tendon rupture is multifactorial. It results from tenosynovial invasion of tendons or, more commonly, from their attrition on the ulnar head. It is a sequential process, beginning from the proper extensor of the fifth finger. Dorsal dislocation of cubital head abrading the overlying tendons especially the tendon of the little finger in the fifth compartment. This, initiate a functional disorder in extensor apparatus, then can and subsequently occurs the rupture of the other tendons in particular the extensor digitorum communis. The lack of association between tendon rupture and wrist pain is consistent with the usual mechanism of rupture, namely attrition on damaged bone rather than invasion by active synovitis. Capsulo-ligamentar tears can aggravate the bone contact with the tendons and accelerate the rupture [1,16-18]. Other tendons can be also, less frequently, ruptured. The extensor policis longus, is commonly altered in rheumatoid arthritis. In this tendon, tenosynovitis in the reflexional zone at the lister tubercule, in addition to hyperpressure and hypovascularization, are the most cause of rupture. Also, in evolutive forms, rupture of the extensor carpi ulnaris accelerate wrist misalignment and can be one factor of other tendon rupture [16]. As mentioned above, mechanical injury is often responsible of tear by altering the tendon along its course over bone or connective tissues. Other pathophysiological mechanisms during the inflammation process are related to action of lysosomal enzymes, released in the connective tissue of the tendon. Ischemic mechanisms can be found in hypertrophic peri-tenosynovitis by constriction of vessels supplying the peritenon. This causes a microvascular response to tissue hypoxia contributing to rupture, and this is probably why in many cases of tendon rupture roughened spurs are not always found [14,19].

• Yellow arrow: Scallop sign.
• There is also a diastasis of distal radioulnar joint.
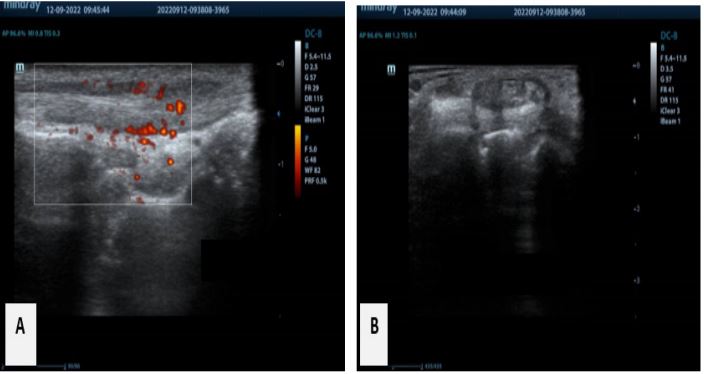
A: Tenosynovitis of extensor digiturum communis with Doppler activity
B: Transversal US section of the 4th and the 5th compartment, with empty synovial sheath of extensor digiti minimi.
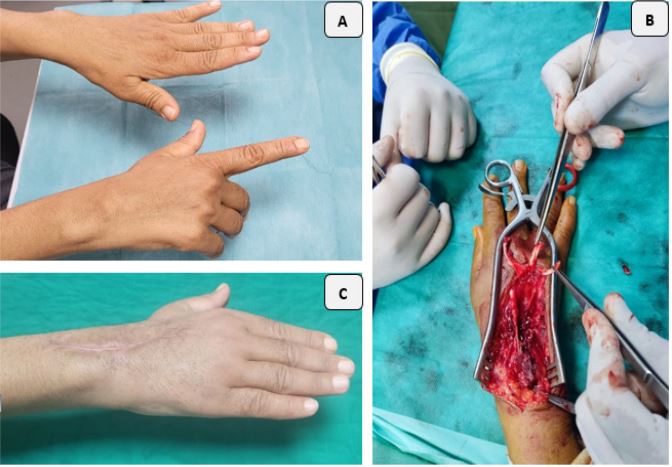
B: Per operative view showing tendons rupture (3th, 4thand fifth tendons)
C: Postoperative results, 2 month later
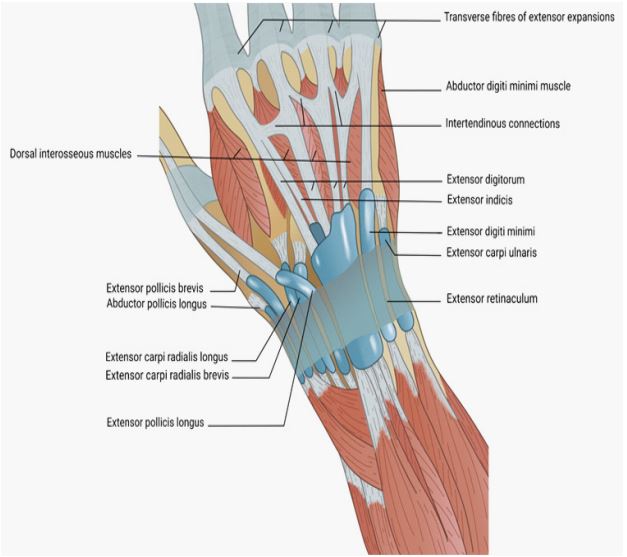
Schemas realized by doctor Mahdi Mohammed Amine According to [3].
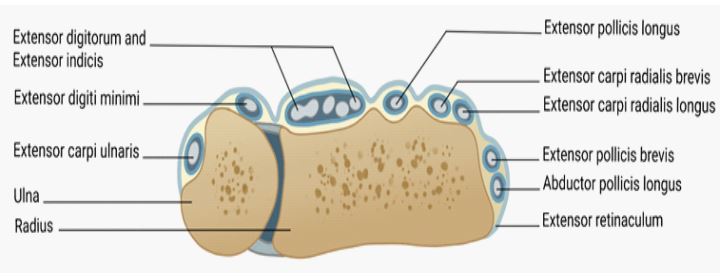
Schemas realized by doctor Mahdi Mohammed Amine According to [3].
Schemas realized by doctor Mahdi Mohammed Amine According to [3].
Risk factors
A spontaneous tendon rupture can appear without any noticeable impact, it can occur without any trauma. Several risk factors can precipitate rupture. In literature, it is mentioned that duration of symptoms is one of these risk factors. An evolution of disease longer than eight year, and a chronic tenosynovitis with persistent inflammation more than year increases the risk of rupture. Also, carpe disorganization, dislocation of ulnar head a scallop sign on X-ray as in our patient and a high Larsen score indicate a higher probability of extensor tendon rupture [20,21]. Despite recent advancement of therapeutics in rheumatoid arthritis, patients with first tendon rupture are still at risk of sequential tendon ruptures. Education of the risks of sequential tendon ruptures and timely consultation to hand surgeons for preventive intervention continue to be an important component of patients care [22].
Prevention
It is evident that the first preventive measure of rupture is to treat well rheumatoid arthritis. The development of targeted biologic medications improved outcomes. Rheumatologists now, by applying a “Treat to Target “(T2T) strategy, aim for remission or Low Disease Activity (LDA) in patients with rheumatoid arthritis. Despite guidelines of T2T approach are available since 2014, the feasibility of using a T2T approach varies from physicians and across countries [23]. So, we still have a structural progression in rheumatoid hand and wrist then still have tendons ruptures.
To preserve hand function before tendon rupture, a collaboration of rheumatologists and hand surgeons must start early. In the presence of risk factors, an early prophylactic extended tenosynovectomy and synovectomy can prevent severe damage of extensor tendon. Also, some prophylactic procedures on soft tissues and carpal bones, can stop or at least slow down the development of severe axial deformities of the wrist and hand which are risk factors of rupture [14,20]. In one study, prophylactic tenosynovectomy and wrist synovectomy were performed on 42 joints in 35 patients. Prophylactic surgery effectively prevented rupture of the tendons in patients who had two or more risk factors for extensor tendon rupture [21]. To be effective as a prophylactic procedure, tenosynovectomy has to be done before there is significant tendon damage. It is usually considered to prevent subsequent tendon rupture and recurrent tenosynovitis [24]. The risk of rupture is virtually eliminated by placing the extensor retinaculum under the extensor tendons of the fingers and thumb. To justify prophylactic surgery in the large group of patients whose symptoms are controlled medically and whose level of risk of tendon rupture is modest, we must have a way to identify patients at high risk. In one study, wrist pain, distal radioulnar crepitus, ulnar head prominence and tenderness are found between one fifth and one third of the wrists studied [17].
Rupture management
The management of rheumatoid arthritis is actually codified. Learned societies in rheumatology frequently updated recommendations to explain therapeutic strategies and drugs choices. The main goal of management is the early diagnosis, the early initiation of effective therapeutics then automatically prevention of structural damages [25-27]. Certainly, tendon rupture occurs in advanced stages of the disease as a complication. As seen above, tenosynovectomy can prevent rupture. If this occurs, surgical repair is required. Early referral to surgeons is also indicated for imminent or actual tendon rupture and nerve compression, to prevent irreversible damage [13].
Tendon repair
To treat these tendon ruptures, several surgical techniques are described. Simple end-to-end suture of the stumps, tendon transfer or tendon grafting are the most used. Simple suture of ends is usually not evident because of poor stumps. So, tendon repair surgery using free grafts or, more often, intact tendon transfer is necessary. Also, tendon transfer and tendon grafting are the preferred methods for repairing extensor tendon rupture because flexion will be limited after resection of damaged stumps if simple end-to-end is done [14,28]. For tendon grafting, some authors have focused on the surgery delay, they suggest that tendon grafting may be possible up to 20 weeks post rupture in rheumatoid patients. Also, in rheumatoid hand, because of multiple tendons damage, the quality of tendon donor can be altered, and also, the quality of healing is not well. Transfer in these situations can be preferred to graft. If grafting is indicated, the choices are multiple. Tendon donors can be palmaris longus, strips of extensor carpi radialis brevis. In the same time, the preexisting rheumatoid synovitis and exposed ulnar head and bony spicules should be addressed surgically before performing a tendon transfer [29]. The extensor tendon reconstruction using autogenous palmaris longus tendon graft achieve good clinical results in one study [30]. In literature, both tendon transfer and tendon graft for extensor tendon rupture in rheumatoid hands achieve favorable long-term outcomes, with no significant differences between the procedures. In cases of tendon graft, the time to surgery should be considered, and there is concern over re-rupture and extension lag of metacarpophalangeal joints [31]. Surgical outcomes in patients with ruptures in 3 fingers were inconsistent compared with those in patients with ruptures in 2 fingers [30].
Conclusion
Rheumatoid arthritis is a frequent rheumatic disease with a major impact on quality of life and high disability if diagnosis and management are delayed. Tendon rupture is one of the frequent complications. Extensor tendon rupture is common in rheumatoid hand because of bony reconstruction in advanced disease. Management of rupture occurs collaboration between surgeons and rheumatologists early when risk factors are present. Surgical techniques have a good outcome, but the complexity is about the quality of tendon structure already altered by inflammation and rheumatoid disorders. So, functional prognosis is not always very well.
Declarations
Acknowledgements: We thank Dr. Mahdi Mohammed Amine for producing the anatomical illustrations in this article.
Support and funding: None.
Conflict of interest: None.
References
- Vaughan-Jackson OJ. Rupture of extensor tendons by attrition at the inferior radio-ulnar joint; report of two cases. J Bone Joint Surg Br. 1948; 30B: 528‑30.
- Biehl C, Rupp M, Kern S, Heiss C, ElKhassawna T, et al. Extensor tendon ruptures in rheumatoid wrists. Eur J Orthop Surg Traumatol. 2020; 30: 1499‑504.
- Atlas of Human anatomy. 2023.
- Masson E. Lésions traumatiques des tendons extenseurs de la main. EM-Consulte. 2022.
- Chick G, Papaloïzos M. 16 - Plaies des tendons extenseurs. In: Chick G, Papaloïzos M, éditeurs. Urgences de la main et du poignet. Paris: Elsevier Masson. 2014; 125-34.
- Colquhoun M, Gulati M, Farah Z, Mouyis M. Clinical features of rheumatoid arthritis. Medicine (Baltimore). 2022; 50: 138‑42.
- Vittecoq O, Kozyreff-Meurice M, Auquit-Auckbur I. Main et poignet rhumatoïdes. Rev Rhum Monogr. 2012; 79: 173‑83.
- Wakefield RJ, Balint PV, Szkudlarek M, Filippucci E, Backhaus M, et al. Musculoskeletal ultrasound including definitions for ultrasonographic pathology. J Rheumatol. 2005; 32: 2485-7.
- Filippucci E, Gabba A, Di Geso L, Girolimetti R, Salaffi F, et al. Hand tendon involvement in rheumatoid arthritis: an ultrasound study. Semin Arthritis Rheum. 2012; 41: 752‑60.
- Elangovan S, Tan YK. The Role of Musculoskeletal Ultrasound Imaging in Rheumatoid Arthritis. Ultrasound Med Biol. 2020; 46: 1841-53.
- Bruyn GAW, Hanova P, Iagnocco A, d’Agostino MA, Möller I, et al. Ultrasound definition of tendon damage in patients with rheumatoid arthritis. Results of a OMERACT consensus-based ultrasound score focussing on the diagnostic reliability. Ann Rheum Dis. 2014; 73: 1929‑34.
- Lillegraven S, Bøyesen P, Hammer HB, Østergaard M, Uhlig T, et al. Tenosynovitis of the extensor carpi ulnaris tendon predicts erosive progression in early rheumatoid arthritis. Ann Rheum Dis. 2011; 70: 2049‑50.
- Wu F, Talwalkar S. Surgical management of the rheumatoid hand and wrist. Orthop Trauma. 2019; 33: 23‑9.
- Pech J, Veigl D, Vlček M. Spontaneous Tendon Ruptures in the Rheumatoid Hand. Acta Chir Orthop Traumatol Cech. 2016; 83: 375-80.
- Shapiro JS. The wrist in rheumatoid arthritis. Hand Clin. 1996; 12: 477‑98.
- Merle M, Jager T, Herzberg G. Poignet rhumatoïde. In: Chirurgie de la Main. Elsevier; 2017; 247-305.
- Williamson L, Mowat A, Burge P. Screening for extensor tendon rupture in rheumatoid arthritis. Rheumatology. 2001; 40: 420‑3.
- Henry J, Roulot É, Gaujoux-Viala C. La main rhumatoïde. Presse Médicale. 2013; 42: 1607-15.
- Sivakumar B, Akhavani MA, Winlove CP, Taylor PC, Paleolog EM, et al. Synovial Hypoxia as a Cause of Tendon Rupture in Rheumatoid Arthritis. J Hand Surg. 2008; 33: 49‑58.
- Hsueh JH, Liu WC, Yang KC, Hsu KC, Lin CT, et al. Spontaneous Extensor Tendon Rupture in the Rheumatoid Wrist: Risk Factors and Preventive Role of Extended Tenosynovectomy. Ann Plast Surg. 2016; 76: S41-47.
- Ryu J, Saito S, Honda T, Yamamoto K. Risk factors and prophylactic tenosynovectomy for extensor tendon ruptures in the rheumatoid hand. J Hand Surg Edinb Scotl. 1998; 23: 658‑61.
- Gong HS, Lee JO, Baek GH, Kim BS, Kim JY, et al. Extensor tendon rupture in rheumatoid arthritis: A survey of patients between 2005 and 2010 at five Korean hospitals. Hand Surg Int J Devoted Hand up Limb Surg Relat Res J Asia-Pac Fed Soc Surg Hand. 2012; 17: 43-7.
- Salomon-Escoto K, Kay J. The “Treat to Target” Approach to Rheumatoid Arthritis. Rheum Dis Clin N Am. 2019; 45: 487‑504.
- Brown FE, Brown ML. Long-term results after tenosynovectomy to treat the rheumatoid hand. J Hand Surg. 1988; 13: 704‑8.
- Ghozlani I. Actualisation des recommandations de la Société Marocaine de Rhumatologie pour la prise en charge de la polyarthrite rhumatoïdeUpdate of Moroccan Society of Rheumatology recommendations for the management of rheumatoid arthritis. 2022.
- Fraenkel L, Bathon JM, England BR, St.Clair EW, Arayssi T, et al. American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis Care Res. 2021; 73: 924‑39.
- Coates L, Gossec L. The updated GRAPPA and EULAR recommendations for the management of psoriatic arthritis: Similarities and differences. Joint Bone Spine. 2023; 90: 105469.
- Wilson RL, DeVito MC. Extensor tendon problems in rheumatoid arthritis. Hand Clin. 1996; 12: 551‑9.
- O’Sullivan MB, Singh H, Wolf JM. Tendon Transfers in the Rheumatoid Hand for Reconstruction. Hand Clin. 2016; 32: 407‑16.
- Lee KH, Jo YH, Kim SJ, Choi WS, Lee CH, et al. Clinical Results of Autogenous Palmaris Longus Tendon Graft for Ruptures of Multiple Extensors in Rheumatoid Hands. J Hand Surg. 2018; 43: 947.e1-947.e9.
- Lee YS, Kim HS, Kim YH, Jo YH, Lee BG, et al. Long-term clinical outcome of tendon transfer and tendon graft for extensor tendon ruptures in rheumatoid hands. BMC Musculoskelet Disord. 2022; 23: 865.