
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Huge right atrial myxoma manifesting with dyspnea and right-sided heart failure: A case report
Maryam Taherkhani, MD1; Houra Yeganegi, MD2*; Ramin Baghai Tehrani, MD3
1Associate Professor of Interventional Cardiology, Loghman Hakim Hospital, Shahid Beheshti University of Medical Science, Tehran, Iran.
2Cardiologist, Clinical Research Development Center of Loghman Hakim Hospital, Shahid Beheshti University of Medical Science, Tehran, Iran.
3Associate professor of Cardiac Surgery, Modarres Hospital, School of Medicine, Shahid Beheshti University of Medical Science, Tehran, Iran.
*Corresponding Author : Houra Yeganegi
Cardiologist, Clinical Research Development Center
of Loghman Hakim Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Email: sarvenaz_yeganegi@yahoo.com
Received : Nov 14, 2023
Accepted : Dec 15, 2023
Published : Dec 22, 2023
Archived : www.jcimcr.org
Copyright : © Yeganegi H (2023).
Abstract
Although cardiac myxomas are the most prevalent type of primary cardiac tumors, barely they originated from the right atrium and generally are asymptomatic in such cases. Here we described a case of a 24-year-old male with right atrial myxoma. The mass was huge and obstructed the tricuspid valve which eventually led to right-sided heart failure. Transthoracic echocardiography revealed the size and position of the mass with good precision. Surgical excision of the neoplastic mass, as the only promising treatment, should be planned immediately after diagnosis.
Keywords: Cardiac myxoma; Heart failure; Right atrium; Surgical excision; Transthoracic echocardiography.
Citation: Taherkhani M, Yeganegi H, Tehrani RB. Huge right atrial myxoma manifesting with dyspnea and right-sided heart failure: A case report. J Clin Images Med Case Rep. 2023; 4(12): 2753.
Introduction
Primary cardiac tumors occur rarely with a prevalence rate of less than 0.03% which are non-cancerous in most cases [1]. Myxomas are the most common cardiac tumors, accounting for about 50% of benign primary cardiac tumors [2]. These tumors commonly occur in females and after the third decade of life [3]. Over 70% of all cardiac myxomas originate from the Left Atrium (LA) and 18% from the Right Atrium (RA) [2]. Common symptoms of myxomas in other organs are systemic embolization, neurological manifestation, and stroke [1,4]. Cardiac manifestations of such tumors include arrhythmia, heart failure, and pericardial effusion [1]. Right atrial myxomas are usually asymptomatic or sometimes present with dyspnea [2]. Although rightsided heart failure occurs very rarely in right atrial myxoma cases, here we report a 24y patient with right atrial myxoma and right-sided heart failure.
Case presentation
A 24 years old male patient was admitted to the emergency room with a history of progressive edema and abdominal distention from 2 weeks ago. He had dyspnea on excretion with New York Heart Association (NYHA) class III to IV in the last 2 weeks and associated with orthopnea.
The past medical history was unremarkable. On physical examination, the patient had elevated neck vein, ascites, and lower limb edema.
Cardiac auscultation revealed a mid-diastolic murmur at the left sternal border. The patient had tachycardia and the blood pressure was 107/75 mm Hg.
Last week he presented to the internist clinic due to limb edema and fatigue. So an approach to generalized edema was done. Laboratory indices including total protein, urine analysis, and thyroid function test (TFT) were unremarkable. Chest X-Ray showed cardiomegaly and right atrial enlargement (Figure 1).

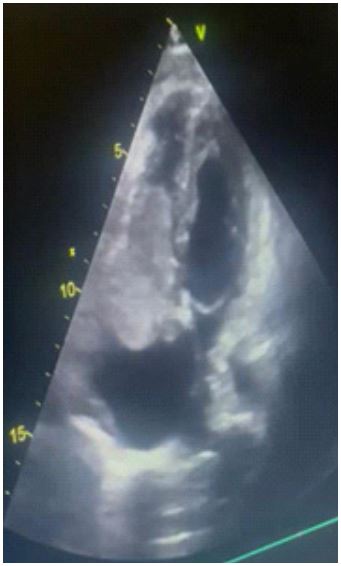
Based on the routine procedure of our center due to the edema and abnormal heart exam, transthoracic echocardiography was done and showed a Left Ventricular Ejection Fraction (LVEF) of 40%, abnormal septal motion due to Right Ventricular (RV) volume overload, and severe Right Atrial (RA) and RV enlargement.
As shown in Figure 2, a large heteroechoic mobile mass was seen in RA (57×46 mm) with an obstructive effect on the tricuspid valve and a compressive effect on the left ventricle.
During this admission, he had 3 episodes of lightheadedness and pre-syncope symptoms when changing position from supine to lateral decubitus. A discussion was held with the cardiothoracic surgery team for emergent surgery. The patient underwent surgical excision of the right atrial mass the following day.
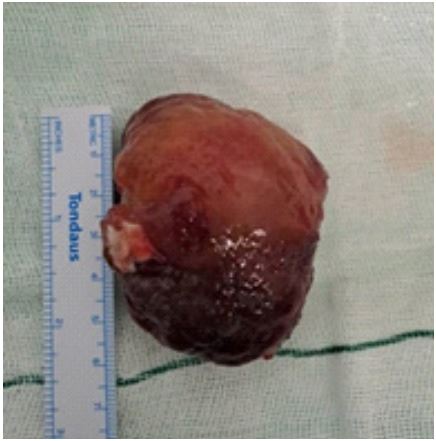
The approach to excision was executed via midline sternotomy, with systemic heparinization and standard aortic and bi-caval cannulation to achieve cardiopulmonary bypass with active cooling to 34°C (Figure 3). As shown in Figure 4, right atriotomy revealed a massive right atrial mass, which was typically pedunculated and manifested as a cavitary gelatinous mass in size of about 6.5×5 cm.
Microscopic examination of cardiac myxoma revealed intratumoral hemorrhage and focal calcification, but the base of the tumor was free of calcification. Histologically cardiac myxomas are mainly composed of stellated fusiform and polygonal cells immersed in an amorphous myxoid stroma.

Discussion
Metastatic cardiac tumors are more common than primary cardiac tumors. Cardiac myxomas are the most common type of primary cardiac tumor. The usual site of involvement is the left atrium, but rarely it involves the right atrium [5]. While in most cases, cardiac myxomas occur in females and usually after the third decade of life, here we presented a 24 years old male patient with a massive atrial myxoma.
The presentation of right atrial myxomas is variable and depends on size, position, mobility of the tumor, and also on the patient body position and physical activity. It can remain asymptomatic or can cause constitutional symptoms as well as dyspnea [6]. Our patient presented with dyspnea for the last two weeks before surgery and experienced right-sided heart failure, which is extremely rare in myxomas.
Right atrial myxomas may obstruct the tricuspid valve, the manifestation of which may be heart failure or even collapse [7,8]. This case illustrates the influence of myxoma’s size, position, and mobility as well as the patient’s complaints and signs. The mass obstructed the tricuspid valve, which probably was the reason for heart failure in this patient. But Chest X-ray and electrocardiography are of limited value in such cases and echocardiography is the gold standard method for the diagnosis of cardiac myxomas. Other imaging modalities like Computed Tomography (CT) scanning and magnetic resonance imaging play an ancillary role [9]. In this case, we used transthoracic echocardiography and a huge echogenic right atrial mass was obvious that obstructed the tricuspid valve.
Currently, there is no effective medical treatment, and surgical excision of the tumor is the treatment of choice that has a low mortality rate (less than 5%) [10]. The surgical excision of cardiac myxoma carries a low-operative risk and gives excellent short- and long-term results [11].
Outcome data on myxomata are limited to case reports and small series. The optimal timing of surgery has not been evaluated systematically. However, death whilst awaiting operation has been reported and so it is logical that especially in the setting of possible outflow tract obstruction, surgical resection should be undertaken as a matter of urgency. In this case, due to the size of the mass and the risks of sudden death due to right ventricular outflow tract obstruction, urgent surgical resection was recommended [12].
Conclusion
Although right atrial myxomas are rare and asymptomatic, the size and the position of the mass may lead to tricuspid valve obstruction and right-sided heart failure. Surgical excision of the neoplastic mass, as the only promising treatment, should be planned immediately after diagnosis is established.
References
- Shrestha S, Raut A, Jayswal A, Yadav RS, Poudel CM. Atrial myxoma with cerebellar signs: A case report. J Med Case Rep. 2020; 14: 29.
- Bonow R, Mann DL, Zipes DP, Libby P. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine. 9th edition. 9 ed. Philadelphia: Elsevier Saunders. 2011.
- Kohno N, Kawakami Y, Hamada C, Toyoda G, Bokura H, et al. Cerebral embolism associated with left atrial myxoma that was treated with thrombolytic therapy. Case Rep Neurol. 2012; 4: 38-42.
- Azdaki N, Moezi S, Hosseinzadehmaleki M, Farzad M. Failed primary percutaneous coronary intervention in a middle-aged man without cardiovascular risk factors: left atrium myxoma. Pan Afr Med J. 2020; 36: 6.
- Reynen K. Cardiac myxomas. N Engl J Med. 1995; 333: 1610-7.
- Nina VJ, Silva NA, Gaspar SF, Raposo TL, Ferreira EC, et al. Atypical size and location of a right atrial myxoma: a case report. J Med Case Rep. 2012; 6: 26.
- Agrawal R, Sharma A, Nath RK, Pandit BN. Massive right atrial myxoma presenting as congestive heart failure: an unusual presentation of a rare tumour. BMJ Case Rep. 2018; 2018.
- Alamri Y, Lau YY, Lainchbury J. Large right atrial myxoma presenting with heart failure. ANZ J Surg. 2019; 89: 1341-2.
- Islam A. Cardiac myxomas: A narrative review. World J Cardiol. 2022; 14: 206-19.
- Agstam S, Kumar B, Dahiya N, Guleria VS. Giant right atrial myxoma presenting as right heart failure: A rare manifestation. BMJ Case Rep. 2020; 13.
- Naser N, Hadziomerovic N, Bahram D, Kacila M, Pandur S. Giant Right Atrial Myxoma with Symptoms of Right Heart Failure. Med Arch. 2021; 75: 66-8.
- Straw S, Sengupta A, Gantenby VK, Schlosshan D, Ferrara A, et al. An enormous right atrial myxoma highlights the role of echocardiography in heart failure pathways: a case report. Eur Heart J Case Rep. 2022; 6: ytac042.