
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 4
Dermatofibrosarcoma protuberans in adult diagnose by a single biopsy
Casper Bo Poulsen1*; Carsten Sauer Mikkelsen2; Luit Penninga3; Peter Bjerring4
1Department of Dermato-Venereology, Aalborg University Hospital, Denmark.
2Specialist in Dermato-Venereology, Private Practice in Dermato-Venereology, Brønderslev, Denmark; Research Lab, Department of Dermato-Venereology, Aalborg University Hospital, Denmark.
3Specialist in Surgery, Phd, Clinical Assoc. Professor, Department of Surgery and Transplantation, Rigshospitalet, Denmark.
4Clinical Professor, Dr.med, Specialist in Dermato-Venereology, Department of Dermato-Venereology, Aalborg University Hospital, Denmark.
*Corresponding Author : Casper Bo Poulsen
Department of Skin and Venereal Diseases, Aalborg
University Hospital, Denmark.
Email: casppu@rm.dk
Received : Nov 14, 2023
Accepted : Dec 15, 2023
Published : Dec 22, 2023
Archived : www.jcimcr.org
Copyright : © Bo Poulsen C (2023).
Abstract
Dermatofibrosarcoma Protuberans (DFSP) is a rare cutaneous sarcoma with an overall incidence of 4.1 cases per million/year according to the largest population-based study of DFSP. This cutaneous sarcoma has an overall ten-year survival of 99.1% [1]. This low-grade malignant sarcoma exhibits slow growth and has low metastatic potential (<3%) but a high rate of recurrence [2]. Disseminated DFSP occurs in 1%-4% of cases and is associated to high mortality with the majority of patient dying within the first two years [3]. Most tumors are located on the trunk with approximately 50% to 60% of all tumors in this region, proximal extremities account for 20%-30% [3].
Clinical presentation of DFSP is a firm, multilobulated tumor, fixed to the skin but not the deeper tissue. Presentation varies a lot due to the slow growth nature of the tumor. The skin may have a red to blue discoloration in most cases [4].
Diagnostics of the clinical presentations is often difficult with multiple differential diagnosis with erythematous and violaceous plaques. Biopsy specimen including subcutaneous tissue is needed to diagnose DFSP histologically and to notice possible sarcomas. Often CD34 immunohistochemical staining is useful for diagnostics since the spindle cells of the tumor has a strong CD34 expression [2].
A previous case rapport of DFSP showed the need for biopsy in order to not misinterpret skin conditions [5].
The Gold standard of DFSP treatment is surgical tumor resection with histopathological negative margins. Therefore, wide local excision is the most common method as well as Mohs Micrographic Surgery (MMS) which have showed the lowest rate of recurrence. Recently tyrosine kinase inhibitors, such as imatinib has shown to be effective for disseminated DFSP [6].
Citation: Bo Poulsen C, Sauer Mikkelsen C, Penninga L, Bjerring P. Dermatofibrosarcoma protuberans in adult diagnose by a single biopsy. J Clin Images Med Case Rep. 2023; 4(12): 2754.
Case presentation
A 71-year-old woman known with chronic urticaria and atopic dermatitis on the feet is referred from general practitioner to a dermatologist for assessment of a 10 mm soft dome-shaped, slightly red tumor with slow evolvement in left popliteal region (Figure 1a & 1b).
Initially the patient underwent surgical excision where the removed tissue was sent to histological examination at the pathological department.
The following result was seen in the tissue:
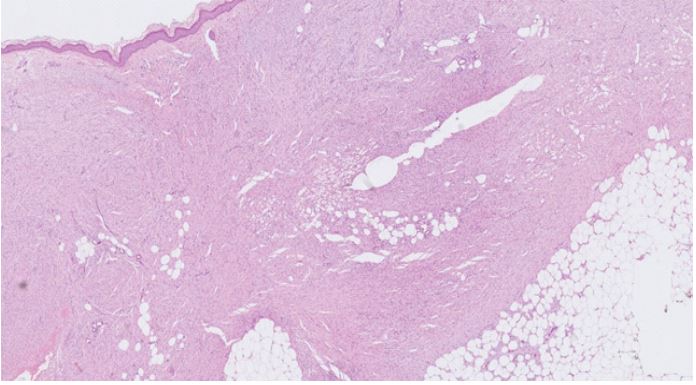
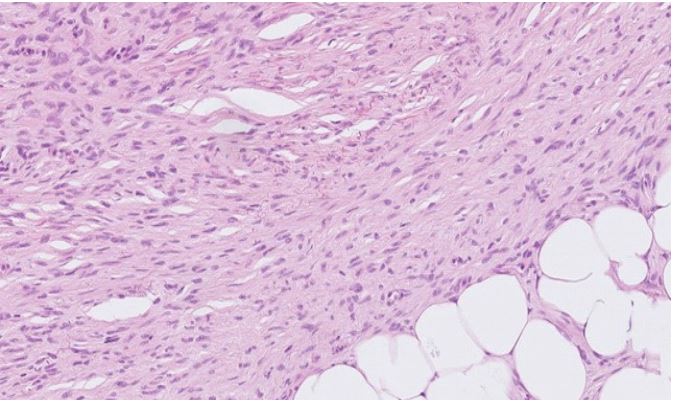
Skin excision including subcutis. In the dermis and subcutis there is a spindle cell neoplasm with a storiform pattern. The tumor cells are ovoid to spindle monomorphic with rare mitotic activity (Figure 2a). There is sparing of adnexal structures and infiltration of the subcutaneous fat in a “honeycomb” pattern (Figure 2b).
Immunohistochemically, the neoplastic cells exhibit diffuse positivity for CD34 and CD10, focal positivity for alpha-smooth muscle actin (ASMA), and they lack expression of Melan-A (MLA), S100, desmin (DES), smooth muscle hamartoma (SMH), anaplastic lymphoma kinase (ALK), and microphthalmia-associated transcription factor (MITF).


Pathological conclusion
Dermatofibrosarcoma protuberans with tumor cells in the surgical margin. Further resection is recommended.
The patient later underwent re-excision by a plastic surgeon and achieved complete excision.
This shows the undoubtable advantage of biopsies in patients with questionable dermatological presentations. Presentation of DFSP in patients primarily on clinical presentation can be extremely difficult. For rapid diagnosis and better treatment, a biopsy is essential.
References
- Dermatofibrosarcoma Protuberans in the United States. Dermatol Surg. 2016; 42: S24-31.
- Llombart B, Serra C, Requena C, et al. Guidelines for Diagnosis and Treatment of Cutaneous Sarcomas: Dermatofibrosarcoma Protuberans. Actas Dermosifiliogr (Engl Ed). 2018; 109: 868-77.
- Gloster HM, Jr. Dermatofibrosarcoma protuberans. J Am Acad Dermatol. 1996; 35: 355-76.
- Taylor HB, Helwig EB. Dermatofibrosarcoma protuberans. A study of 115 cases. Cancer. 1962; 15: 717-25.
- Arvesen KB, Mikkelsen CS, Steiniche T, et al. Dermatofibrosarcoma protuberans diagnosed by a single biopsy. Dermatol Reports. 2012; 4: e10.
- Allen A, Ahn C, Sangüeza OP. Dermatofibrosarcoma Protuberans. Dermatol Clin. 2019; 37: 483-8