
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Juvenile reccurent parotitis: A case report
Ossama Labib*
Derb Ghalf Agency Inwi Residence Falah, Morocco.
*Corresponding Author : Ossama Labib
Derb Ghalf Agency Inwi Residence Falah, Morocco.
Email: oussama1labib@gmail.com
Received : Nov 20, 2023
Accepted : Dec 19, 2023
Published : Dec 26, 2023
Archived : www.jcimcr.org
Copyright : © Labib O (2023).
Citation: Labib O. Juvenile reccurent parotitis: A case report. J Clin Images Med Case Rep. 2023; 4(12): 2757.
Introduction
CJRP is one of the many causes of chronic parotitis in childhood [1]; it is physiopathology remains uncertain. There is no consensus in the management of JRP, and because it is a rare disease, few cases have been reported in the literature to shed light on this entity. The frequency of episodes can vary widely between patients, and understanding why it resolves in puberty is unknown.
Case presentation
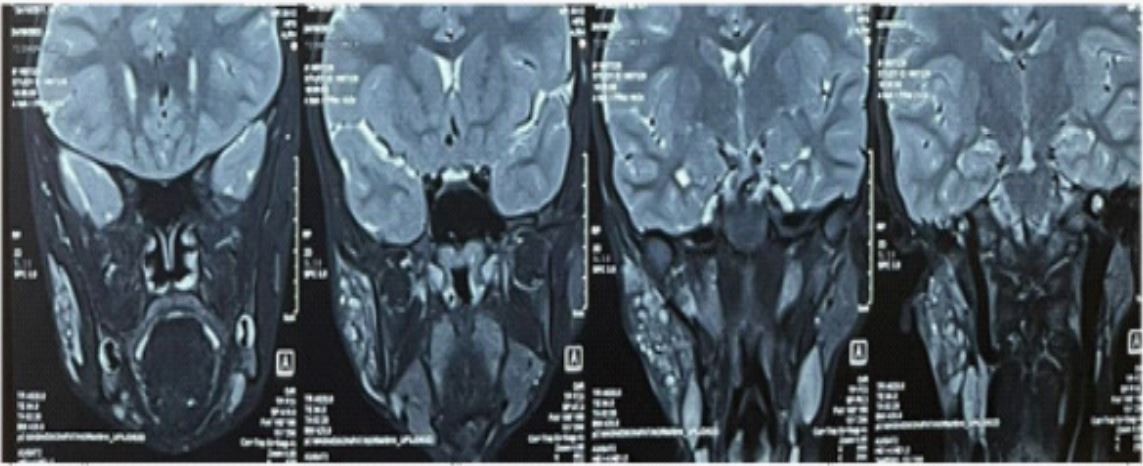
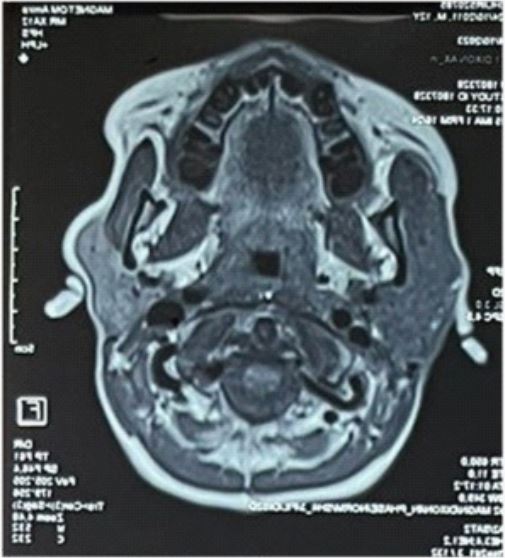
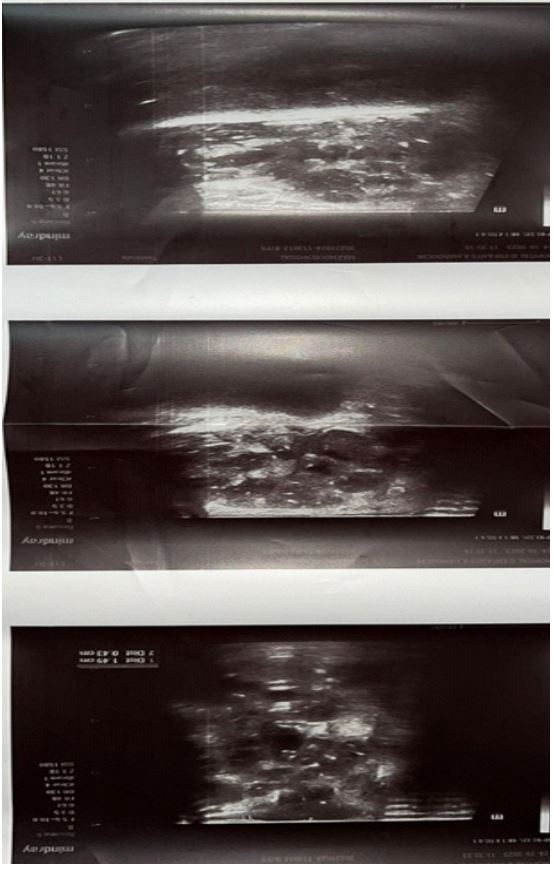
We present the case of an 11-year-old girl with a medical history of recurrent swelling of the right parotid gland for the last 4 years admitted to our emergency department for another episode of painful swelling of the right parotid with a fever at 39 Celsius and alteration of the general state. The physical examination exhibited a painful swelling of the right parotid with reddish overlying skin with no associated facial palsy nor cervical lymphadenopathies; the buccal examination exhibited a normal aspect of the saliva expressed for the Stenson’s duct and normal dental status. The initial management consisted of white cell count which was elevated and elevated C-reactive protein, a negative mumps serology, a negative autoimmune panel, and a US exam showed multiple hypoechoic lesions and heterogeneous echogenicity. We completed it later with an MRI showing multiple communicating intraglandular formations with a liquid signal corresponding to diffuse sialectasis with a peripheral enhancement of a few of these ductal ectasias. Due to its recurrent nature, the age, the negative serologies, and the aspect on both the US and MRI, the diagnosis of Juvenile Recurrent Parotitis was retained. Initially, the management was conservative, and the patient was put on oral analgesics and anti-inflammatory drugs to ease the pain, and an initial antibiotherapy consisted of 6 days of amoxicillin clavulanic acid. The patient was reviewed one week later with significant clinical improvement, the patient was notified with the recurrent nature of the disease the possible occurrence of other acute episodes of painful swelling, and the importance of close follow-up to explore other therapeutical methods if needed in the future.
In the latter six months, the patient exhibited four spells of acute painful swelling with a severe alteration of the QoL with parents noting the onset of a depressive manner in the child with a tendency to isolation, which motivated us to discuss other therapeutical choices. One month later, our patient benefited from sialendoscopy with intraductal injection of steroids and antibiotics showing more arguments in favor of JRP as ductal scaring, the presence of multiple mucus plugs. The close followup at three months was normal. The patient exhibited no other acute spells of swelling and was advised to hydrate well, chew gum, and massage the parotid gland occasionally.
Discussion
JRP is a rare form of parotid inflammation in children [2]. It is characterized by recurrent episodes of painful parotid swelling, often associated with fever and malaise [2]. The first episode typically occurs between the ages of 3 and 6 years (range, six months to sixteen years) more often in males [3]. The etiopathology of juvenile parotitis remains obscure [3]. The most widely accepted theories try to solve this affection by reducing the salivary flow that conditions abnormalities in the structure of distal ducts and predisposes to recurrent inflammation in the gland [5]. Histologically, there are intraductal cystic dilatations of peripheral ducts with periductal lymphocytic infiltration, called sialectasis. The ectatic ducts are usually 1 to 2 mm in diameter and typically have a white appearance of the ductal layer without healthy blood vessel coverage; compared with a normal gland, this aspect is believed to be characteristic of JRP [6] .
The diagnosis is based on the clinical picture and can be confirmed by an ultrasonographic (US) study [4]. At this diagnostic procedure, typical findings are distal small roundish hypoechoic areas in the glandular parenchyma, corresponding to ductal dilatation, duct lymphocytic peripheral infiltration, or enlarged intraparenchymal lymph nodes [4]. Two MRI patterns have been identified as typical of juvenile recurrent parotitis: a T1- weighted hypointense and T2-weighted hyperintense signals, with contrast enhancement, in the acute inflammatory stage, and a T1-weighted and T2-weighted isointense signal, without contrast enhancement, in comparison with the other major salivary glands, in the chronic inflammatory [3,7].
Singh et al. considered sialendoscopy as their main mean of diagnosis in their series [8] due to generalized ductal stenosis, which was noted in the endoscopy procedure [8]. The most recognized sialendoscopy finding was represented by a pale, avascular, and stenotic stenson duct [9]. Nahieli et al. demonstrated the diagnostic value of sialendoscopy by visualizing strictures, hypovascularization, and white intraductal debris, which are characteristic of this disease [10]. They also demonstrated the therapeutic efficacy of concomitant intraductal hydrocortisone lavage, with a 1-year recurrence-free rate of 89%.
Grande-Moreillo et al. concluded in their study that there was a significant difference in the number of inflammation episodes before and after sialendoscopy irrigation in their 9 cases of JRP [11].
Conclusion
Juvenile recurrent parotitis is a rare entity that is often seen in children before the age of puberty, its cause is not quite elicited, and the diagnosis is retained on both clinical and specific findings on both MRI and ultrasound.
References
- Wood, J., Toll, E. C., Hall, F., & Mahadevan, M. (2021). Juvenile recurrent parotitis: Review and proposed management algorithm. International Journal of Pediatric Otorhinolaryngology,142, 110617.
- Garavello, W., Redaelli, M., Galluzzi, F., & Pignataro, L. (2018). Juvenile recurrent parotitis: A systematic review of treatment studies. International Journal of Pediatric Otorhinolaryngology,112, 151-157.
- Capaccio P, Sigismund PE, Luca N, Marchisio P, Pignataro L. Modern management of juvenile recurrent parotitis. J Laryngol Otol. 2012 Dec;126(12):1254-60.
- Berlucchi, M., Rampinelli, V., Ferrari, M., Grazioli, P., & Redaelli De Zinis, L. O. (2018). Sialoendoscopy for treatment of juvenile recurrent parotitis: The Brescia experience. International Journal of Pediatric Otorhinolaryngology, 105, 163-166.
- Miziara, I. D., & Campelo, V. E. S. (2005). Infantile recurrent parotitis: Follow up study of five cases and literature review. Brazilian Journal of Otorhinolaryngology, 71(5), 570-575.
- Tomar, R., Vasudevan, R., Kumar, M., & Gupta, D. (2013). Juvenile recurrent parotitis. Medical Journal Armed Forces India,70(1), 83-84.
- Huisman TA, Holzmann D, Nadal D (2001) MRI of chronic recurrent parotitis in childhood. J Comput Assist Tomogr 25:269– 273.
- Singh, P.P., Goyal, M. & Goyal, A. Sialendoscopic Approach in Management of Juvenile Recurrent Parotitis. Indian J Otolaryngol Head Neck Surg 69, 453–458 (2017).
- Ried E, Douglas F, Crow Y, Hollman A, Gibson J (1998) Autosomal dominant juvenile recurrent parotitis. J Med Genet 35(5):417–419
- Nahlieli, O., Bar, T., Shacham, R., Eliav, E., & Hecht-Nakar, L. (2004). Management of chronic recurrent parotitis: Current therapy. Journal of Oral and Maxillofacial Surgery, 62(9), 1150-1155.
- Grande-Moreillo, C., Margarit-Mallol, J., Fuentes-Carretero, S., Torolla, A., Martí-Camps, M., & Rodríguez-Molinero, A. (2022). Parotid irrigation: A promising option for juvenile recurrent parotitis. American Journal of Otolaryngology, 43(3), 103398.