
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
A rare case of primary gallbladder hydatid disease
Prachi Shukla1; Manish Agrawal2; Simran3; Navdeep Kaur4*
1Assistant Professor, M.G.M & M.Y Hospital, Indore, India.
2Consultant Radiologist, Gokuldas Hospital, Indore, India.
3SHO Gokuldas Hospital, Indore, India.
4Resident Doctor, M.G.M & MY Hospital, India.
*Corresponding Author : Navdeep Kaur
Resident Doctor, M.G.M & MY Hospital, India.
Email: nkaur9176@gmail.com
Received : Nov 22, 2023
Accepted : Dec 20, 2023
Published : Dec 27, 2023
Archived : www.jcimcr.org
Copyright : © Kaur N (2023).
Abstract
Hydatid disease is a parasitic infection caused by echinococcus, mainly echinococcus granulossus. The liver and lungs are the most common sites affected. Primary hydatid gall bladder disease (PHGB) is a rare condition; till now, only 11 cases of PHGB have been reported.
A 32-year-old female presented with severe right upper quadrant abdominal pain from past two months. Routine blood investigations were done, which indicated obstructive jaundice. Imaging investigations like USG, MRI, and MRCP, revealed acute calculus cholecystitis along with PHGB.
The patient underwent cholecystectomy, and the specimen was sent for histopathological examination, and it was proven to be chronic cholecystitis with an Echinococcus granulossus infection of the gall bladder.
Due to its uncommon nature, we rarely consider PHGB as a differential diagnosis. Therefore, careful attention is required to make the diagnosis preoperatively, leading to the appropriate treatment.
Citation: Shukla P, Agrawal M, Simran, Kaur N. A rare case of primary gall bladder hydatid disease. J Clin Images Med Case Rep. 2023; 4(12): 2760.
Case report
A 32 year old female presented to surgical outpatient department with complaint of right upper quadrant abdominal pain from past 2 months. Patient also had complaints of vomiting and itching all over the body. No other significant complaints like fever or chills were present.
Routine investigations were planned which included complete blood count, liver function test, serum bilirubin and urine routine microscopy.
CBC revealed increased neutrophil counts suggesting towards infective etiology.
Liver function test depicted raised SGOT ,SGOT and ALP values (SGOT-225 U/L SGPT 349 U/L ALP-438 U/L). Total Serum bilirubin was 2.8 mg/dl and direct bilirubin was 1.8 mg/dl.
Bile salts and bile pigments were found positive in urine examination.
Clinical picture of jaundice with right upper quadrant pain along with findings of blood and urine investigations pointed towards obstructive pathology related to biliary system.
Patient was referred to radiology department for ultrasonography of whole abdomen.
Chest X-ray was found normal (Figure 1) and did not reveal any focal lesion.
The USG report revealed that gall bladder was found distended with evidence of multiple tiny calculi of 6-8 mm in size at fundus of gall bladder with gall bladder wall appeared thickened and oedematous. Rest of the organs were found normal and the diagnosis of acute calculus cholecystitis was made.
MRI of the abdomen and MRCP were performed and the liver was found mildly enlarged measuring approximately 17.5 cm in the midclavicular line and revealed hepatic steatosis. No focal parenchymal lesion was seen in liver.
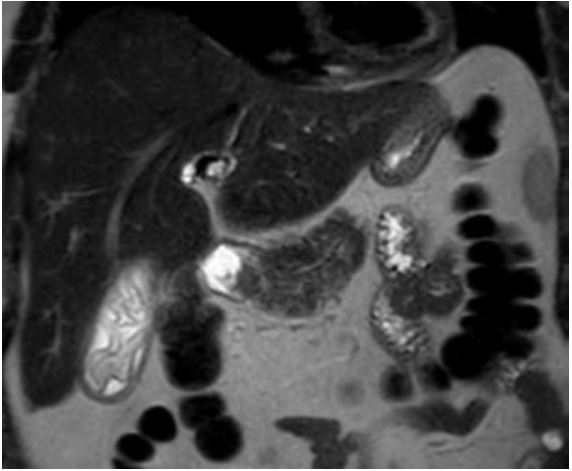
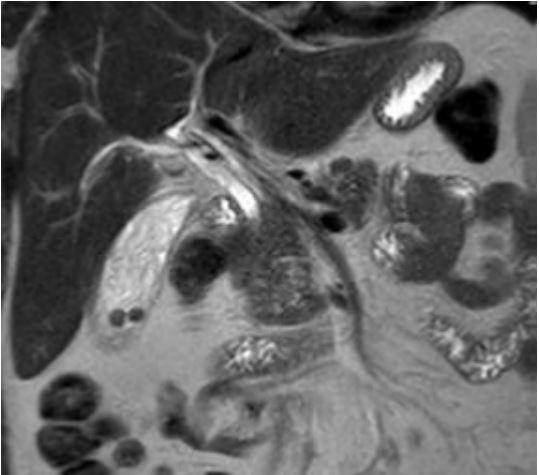
The gall bladder was distended and revealed multiple hyperintense calculi in the dependent portion of its fundus and mild circumferential wall thickening and edema changes, suggesting changes of acute calculus cholecystitis (Figure 2). There was evidence of curvilinear membranous crumpled intensity within the gallbladder lumen and in the common bile duct on the T2Wt images (Figures 3 and 5).
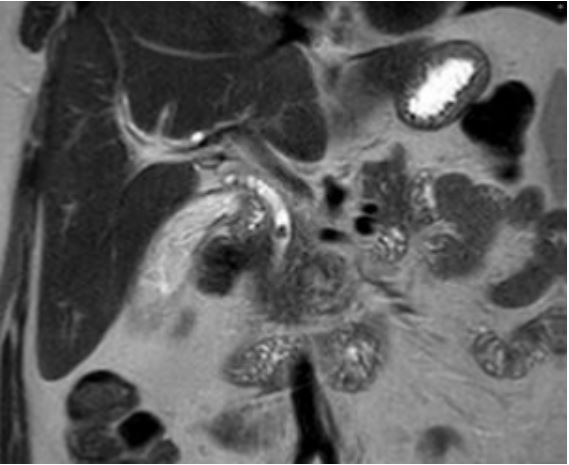
There was no intra or extrahepatic biliary radical dilatation on MRCP images. A small intraluminal calculus of approx. 5mm was seen in the middle 1/3rd of common bile duct located approximately 2.7 cm proximal to its biliary opening (Figure 4).
Rest of the solid organs were found normal and no other significant abnormality was found.
There was no free fluid or enlarged lymph node in the abdomen or pelvis. The final impression was acute calculus cholecystitis with choledocholithiasis with? GB hydatid disease. Patient underwent cholecystectomy and the sample was sent for histopathological examination.
On the Histopathological examination sections showed variable amounts of predominantly mononuclear inflammatory infiltrate predominantly consisting of T lymphocytes, some plasma cells, histiocytes and occasional eosinophils and hypertrophy of muscularis and variable degrees of mural fibrosis, elastosis, neural hyperplasia was noted. Abundance of ovoid shaped protoscolices containing hooklets, sucker and lamellated membranous structures was seen which were very well suggestive of Echinococcus granulossus.
Final impression of Chronic lympho-plasmacytic cholecystitis with Echinococcus Granulosus (Hydatid disease) was made.

Discussion
Etiology and demographics
Hydatid disease has been acknowledged as an important clinical entity since ancient times. The disease is a serious problem in India, where it is endemic and is found in all age groups, gall bladder hydatid disease is more common in adulthood. Hydatid disease is a parasitic infection caused by echinococcus, mainly echinococcus granulossus. The liver and lungs are the most common sites affected. Primary hydatid gall bladder disease (PHGB) is a rare condition; till now, only 11 cases of PHGB have been reported.
The parasite is found in the small intestine of the definitive hosts like dogs and foxes and is transmitted to the intermediate hosts such as sheep and humans by ingestion of ova in feces. After ingestion, the embryonic form of the parasite passes to the liver via the portal vein. If it escapes trapping in the liver, most frequent location is the lung (second filter). If the embryos escape the liver and lung filters or by-pass them via lymphatics, this results in hematogenous and lymphatic dissemination. Thereafter, the embryo can lodge in any part of the body and develop into the larval stage.
Atypical locations reported for hydatid cyst include the spleen, kidney, peritoneum, retroperitoneum, pancreas, gallbladder, inguinal region, cerebral hemispheres, spinal cord, mediastinum, and seminal vesicle.
Clinical and imaging findings
Hydatid disease in gall bladder usually remains asymptomatic or may present with pain localized in right upper quadrant or rarely in epigastrium. Jaundice may occur by the compression of the common bile duct by hydatid cyst or after migration of daughter cyst in biliary tract. In our case patient presented with similar complaints of right upper quadrant pain and jaundice.
Ultrasonography is first investigation performed when we suspect pathology related to gall bladder and biliary tree. Ultrasonography though useful in diagnosing gall bladder pathologies like cholelithiasis, cholecystitis, gall bladder polyp and others with high accuracy, is less sensitive for gall bladder hydatid disease. Ultrasonography may demonstrate floating membrane, and debris in gall bladder which are easily confused with sludge and can lead to false diagnosis.
CT scan can detect gall bladder stones and its inflammatory, neoplastic and other complications like gall bladder perforation or bile duct pathologies but is not very useful in making accurate diagnosis of gall bladder hydatid disease.
MRI is the investigation of choice, It demonstrates floating membrane, debris and cystic contents (daughter cysts) and can reveal reactive inflammatory changes in the wall of gall bladder. As in this case, MRI abdomen with MRCP demonstrates the wavy undulating curvilinear membranous crumpled intensity within the gallbladder lumen and in the common bile duct, with no evidence of liver involvement.
Final confirmation is done by histopathological examination.
Treatment and prognosis: Extra hepatic hydatid cyst has favourable outcome unless there is rupture of cystic contents which is complicated by peritonitis. Gall bladder hydatid is treated by open /laproscopic cholecystectomy as in this case.
Teaching points: Primary GB hydatid is a relativelty rare disease and is often missed on clinical diagnosis. USG though sensitive in picking up pathologies like gall bladder stones and inflammation can only raise suspicion towards hydatid disease, but MRI and MRCP are investigation of choice and can demonstrate either daughter cysts within GB or floating wavy undulating membrane within it along with feature of cholecystitis.
Confirmatory diagnosis of GB hydatid is made by histopathological examination.
Final diagnosis: Hydatid of gall bladder with chronic inflammatory changes.
References
- Budke CM, Deplazes P, Torgerson PR. Global socioeconomic impact of cystic echinococcosis. Emerg Infect Dis. 2006;12:56–64. doi:10. 3201/eid1
- Mushtaque M, Mir MF, Malik AA, Arif SH, Khanday SA, Dar RA. Atypical localizations of hydatid disease: experience from a single institute. Niger J Surg. 2012;18(1):2–7. doi:10.4103/1117-6806.95466
- Safioleas M, Stamoulis I, Theoqaris S, Moulakakis K, Makris S, Kostakis A. Primary hydatid disease of the gallbladder: a rare clinical entity. J Hepatopancreat Surg. 2004;11:352–356. 7
- Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that eval- uate health care interventions: explanation and elaboration. PLoS Med. 2009;6:e1000100. doi:10.1371/journal.pmed.1000100
- Uzunoglu M, Altintoprak F, Dikicier E, Zengin I, Celik A. Hydatid disease in the gallbladder: a rare location. J Med Cases. 2016;7 (12):522–523. doi:10.14740/jmc2501w
- Kabiraj P, Kuiri SS, De U. Primary hydatid cyst of gallbladder: a case report. Int J Case Rep Images. 2015;6(7):440–443. doi:10.5348/ijcri- 201574-CR-10535
- Noomene R, Ben Maamer A, Bouhafa A, Haoues N, Oueslati A, Cherif A. Primary hydatid cyst of the gallbladder: an unusual locali- zation diagnosed by magnetic resonance imaging (MRI). Pan Afr Med J. 2013;14:15. doi:10.11604/pamj.2013.14.15.1424
- Rabbani K, Narjis Y, Louzi A, Benelkhaiat R, Jalal H, Finech B. Unusual localization of hydatidosis: hydatid cyst of gallbladder. Ann Tropical Med Pub Health. 2011;4:119–121. doi:10.4103/1755- 6783.85766
- Krasniqi A, Limani D, Gashi-Luci L, Spahija G, Dreshaj IA. Primary hydatid cyst of the gallbladder: a case report. J Med Case Rep. 2010;4:29. doi:10.1186/1752-1947-4-29
- Pitiakoudis MS, Tsaroucha AK, Deftereos S, Laftsidis P, Prassopoulos P, Simopoulos CE. Primary hydatid disease in a retroplaced gallbladder. J Gastrointestin Liver Dis. 2006; 15:383–385.
- Wani RA, Malik AA, Chowdri NA, Wani KA, Naqash SH. Primary extrahepatic abdominal hydatidosis. Int J Surg. 2005;3:125–127. doi:10.1016/j.ijsu.2005.06.004.