
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Cliniacal Image - Open Access, Volume 4
Granulomatosis with polyangiitis
Taylor Loon, MBBCh1*; Bianca Vescio2; Joel Woodley-Cook, MBBCh3
1SUNY Upstate Medical University, Syracuse, NY, USA.
2Royal College of Surgeons in Ireland, Dublin, Ireland.
3University of Toronto, Toronto, ON, Canada.
*Corresponding Author : Taylor Loon
SUNY Upstate Medical University, Syracuse, NY,
USA.
Email: loont@upstate.edu
Received : Nov 25, 2023
Accepted : Dec 22, 2023
Published : Dec 29, 2023
Archived : www.jcimcr.org
Copyright : © Loon T (2023).
Citation: Loon T, Vescio B, Woodley-Cook J. Granulomatosis with polyangiitis. J Clin Images Med Case Rep. 2023; 4(12): 2767.
Case description
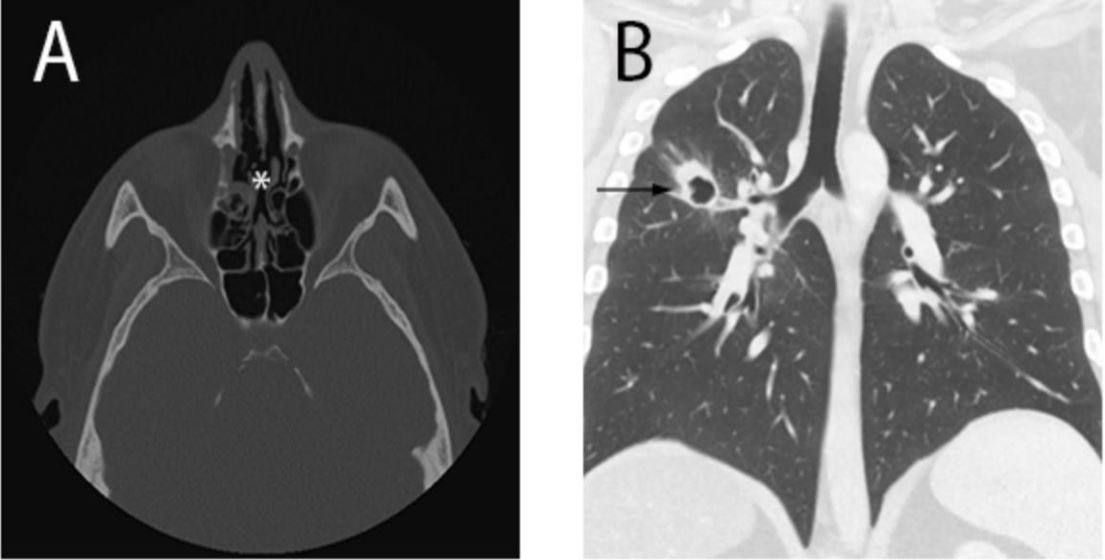
A 30 year old male presented to the emergency department with a 6 month history of hemoptysis and epistaxis. He was otherwise healthy with no known medical conditions, no prior surgery, and was taking no medications. His vital signs were normal and his oxygen saturation was 99% SaO2 on room air. On physical examination he had faint rales within the right upper lobe. Computed tomography scans of the maxillofacial bones and thorax were performed showing perforation of the nasal septum and a right upper lobe cavitary pulmonary lesion.
On laboratory investigations, his leucocyte level was 13.3x109 /L (normal 4-11), neutrophils 9.9x109 (2-7.5) monocytes 1.06x109 (0.2-0.8) with a normal lymphocyte level. There was also an elevated ESR of 10 mm/hr (1-7) with a normal CRP. He had a positive serum C-ANCA. The patient was subsequently diagnosed with Granulomatosis with Polyangiitis and started on treatment with cyclophosphamide and glucocorticoids.
Discussion
Granulomatosis with Polyangiitis (GPA) is an autoimmune medium and small-vessel vasculitis characterised by necrosis and granulomatous inflammation [1]. It anti-neutrophil cytoplasmic antibody (ANCA)-associated which involves both the kidneys respiratory tracts [2]. It is believed to be autoimmune in origin and triggered by environmental events. It predominantly affects Caucasians but occurs in all racial groups [1]. The mean age at diagnosis is 40 but affects a wide age range (8-99 years) [1]. Diagnosis for GPA is based on clinical that is suggestive of vasculitis, positive c-ANCA serology and histological evidence of necrotizing vasculitis, granulomatous inflammation from a biopsy of kidneys, skin or lung, or necrotizing glomerulonephritis [1]. Due to the predominance of thoracic involvement, chest radiology findings frequently suggest diagnosis first. For diagnosis and surveillance of the disease, CT is the choice imaging modality [3]. Findings on chest CT include consolidation, ground-glass opacities, cavitations, masses and nodules [3]. The standard treatment of GPA is a combination of glucocorticoids and cyclophosphamide.
Ethical approval: Written informed consent was obtained from the patient described in this article.
The manuscript has been read and approved by all the authors, and the requirements for authorship in this document have been met, and that each author believes that the manuscript represents honest work.
References
- Greco A, Marinelli C, Fusconi M, Macri GF, Gallo A, De Virgilio A, et al. Clinic manifestations in granulomatosis with polyangiitis. Int J Immunopathol Pharmacol. 2016; 29(2): 151-9.
- Pan L, Yan JH, Gao FQ, Li H, Han SS, Cao GH, et al. Case report of a 28-year-old man with aortic dissection and pulmonary shadow due to granulomatosis with polyangiitis. BMC Pulm Med. 2019; 19(1): 122.
- Martinez F, Chung JH, Digumarthy SR, Kanne JP, Abbott GF, Shepard J-AO, et al. Common and Uncommon Manifestations of Wegener Granulomatosis at Chest CT: Radiologic-Pathologic Correlation. RadioGraphics. 2012; 32(1): 51-69.