
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Primary seminal vesicle schwannoma: Case report with comprehensive review
Naveen Kumar Kushwaha1*; Harish S2; Niharika Mishra3
1Senior Resident (Surgical Oncology), Army Hospital (Research & Referral), New Delhi, India.
2Professor (Surgical Oncology), Army Hospital (Research & Referral), New Delhi, India.
3Postgraduate Resident (Pathology), Army Hospital (Research & Referral), New Delhi, India.
*Corresponding Author : Naveen Kumar Kushwaha
Senior Resident (Surgical Oncology), Army Hospital
(Research & Referral), New Delhi, India, 110010.
Address: MDTC, AH(R & R), Delhi Cantt, New Delhi
110010, India.
Email: nk8844@gmail.com
ORCID ID: 0000-0001-9733-0257
Received : Nov 27, 2023
Accepted : Dec 22, 2023
Published : Dec 29, 2023
Archived : www.jcimcr.org
Copyright : © Kushwaha NK (2023).
Abstract
Schwannomas are rare in seminal vesicles, with most masses being contiguous invasion from nearby malignancies. We report a case of a 23-year-old male with a 7 x 4.6 x 3.5 cm left seminal vesicle mass, confirmed by MRI and biopsy as a low-grade spindle cell neoplasm with neural differentiation. Surgical resection followed by histopathological examination showed a schwannoma arising from the seminal vesicle. Only 16 cases of primary seminal vesicle schwannoma have been reported, emphasizing the need for preoperative histopathological diagnosis prior to definitive management. No optimal surgical approach has been established, but transvesical and laparoscopic methods minimize complications.
Keywords: Seminal vesicle; Schwannoma; Magnetic resonance imaging; Systemic lupus erythematosus; Laparotomy.
Abbreviations: MRI: Magnetic resonance imaging; PSA: Prostate specific antigen; CT: Computed tomography; TRUS: Transrectal ultrasound; SMA: Smooth muscle actin; EMA: Epithelial membrane antigen
Citation: Kushwaha NK, Harish S, Mishra N. Primary seminal vesicle schwannoma: Case report with comprehensive review. J Clin Images Med Case Rep. 2023; 4(12): 2769.
Introduction
Seminal vesicle tumors are usually caused by contiguous invasion from adjacent organ malignancies, such as prostate, rectum, or bladder. Primary tumors of the seminal vesicle are rare and often discovered incidentally [1]. Schwannoma, a slowgrowing benign peripheral nerve sheath tumor composed of Schwann cells, is typically found in the head, neck, mediastinum, and retroperitoneum, and typically diagnosed in individuals aged 30-60 years [2]. Seminal vesicle schwannomas are usually asymptomatic but can cause symptoms due to compression of adjacent structures. Surgical intervention is necessary for symptomatic patients. Tumors that are incompletely resected have a recurrence rate of 30-40%, while malignant transformation is rare [3].
Case report
A 23-year-old male with systemic lupus erythematosus was diagnosed with a left seminal vesicle mass on CT, presenting with minor discomfort during defecation. A digital rectal examination revealed an extra luminal palpable mass along the rectum’s anterior and left lateral wall, while urinalysis and PSA levels were unremarkable. There was no contributory family history.
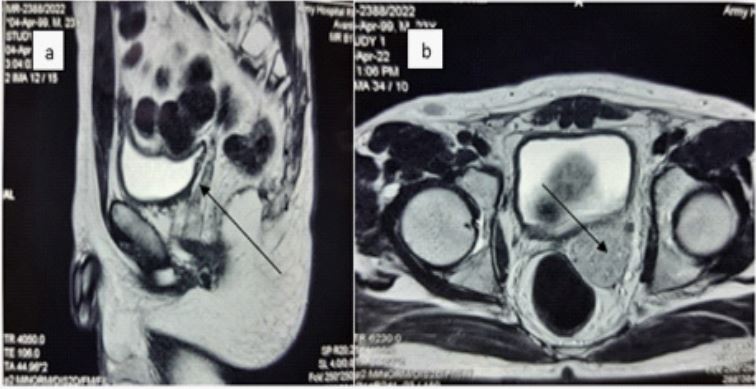
Contrast-enhanced pelvic CT revealed a poorly enhancing, lobulated lesion measuring 7 x 4.6 x 3.5 cm on the left side of the rectovesical space, which seemed to originate from the left seminal vesicle without any discernible cleavage. The lesion was found to be in close proximity to the urinary bladder anteromedially and the rectum posteriorly. Subsequently, a contrast-enhanced pelvic MRI was performed and it confirmed the presence of a left seminal vesicle mass along with small nearby lymph nodes (Figure 1). A low-grade spindle cell neoplasm with neural differentiation was confirmed on histopathological examination following a transrectal ultrasound-guided seminal vesicle biopsy.
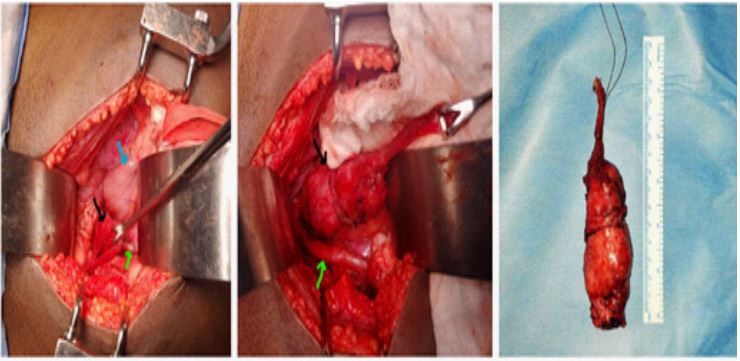
The patient underwent a midline laparotomy of the lower abdomen, which revealed a 9 x 4 cm extraperitoneal mass in the rectovesical space. The pelvic peritoneum was dissected to identify the left ureter and iliac vessels, and upon incision, the tumor was located on the left side of the bladder, with an intact capsule and no adhesion to surrounding structures (Figure 2). The left Vas deferens was transected, and the tumor and left seminal vesicle were removed while preserving the neurovascular structures to the bladder and pelvic wall. The patient had an uneventful post-operative recovery and was discharged on the 5th day. At a 3-month follow-up, the patient’s erectile and ejaculatory functions were normal, and no adjuvant treatment was recommended.
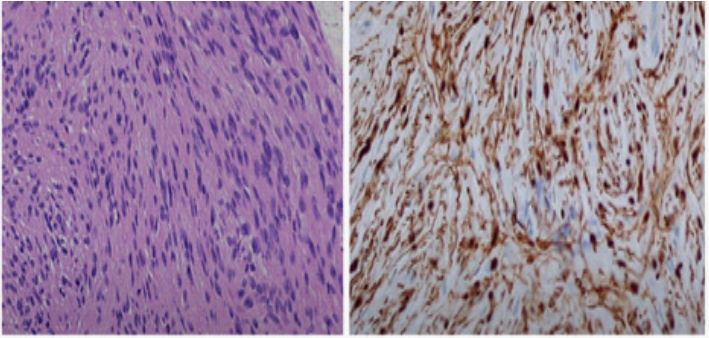
Surgical histopathology revealed a 9 x 3.5 x 2.5 cm left seminal vesicle mass with a 5 cm attached vas deferens. On the cut section, a yellow nodular growth measuring 2.5 x 2 x 2 cm without haemorrhagic or necrotic areas was seen. Microscopic examination showed a low-grade spindle cell tumor with Antoni B and Antoni A areas with verocay bodies. Immunohistochemical analysis confirmed it as a schwannoma from the left seminal vesicle with vimentin, S-100 positive, and Ki 67 <2% (Figure 3).
Discussion
Adenocarcinoma is the most common primary malignancy of seminal vesicles. Primary seminal vesicle Schwannomas are even rarer. Symptoms, when present, are consequent to organ or nerve compression resulting in bladder, ejaculatory or intestinal (rectal) obstruction. Rarely, patients may present dysuria, haematuria or hematospermia and/or pelvic or perineal pain [4].
PubMed and Google scholar search using following terms: “Primary schwannoma of seminal vesicle” OR “Seminal vesicle tumors: schwannomas” OR “Neurogenic tumors of seminal vesicle” OR “Benign schwannoma of the seminal vesicle” OR “Primary solitary schwannoma of the seminal vesicle” OR “Case report and case series of primary schwannoma of seminal vesicle” OR “Immunohistochemical analysis of seminal vesicle schwannoma” revealed that there are very few case series and less than 50 case reports published so far [1-5].
Diagnosing primary seminal vesicle tumors involves ruling out infiltration by surrounding malignancy, with unclear recommendations regarding preoperative biopsy. Imaging findings such as TRUS, MRI, and CT guide diagnosis and surgical management, with contrast-enhanced MRI being the preferred diagnostic method. However, histopathological examination is necessary for definitive diagnosis. Preoperative histopathological diagnosis is crucial for optimal surgical management due to differing approaches for malignant and benign pathologies.
Surgical resection is the curative treatment for benign seminal vesicle tumors, with asymptomatic cases being successfully observed according to reports. Various surgical approaches, including transperitoneal, transcoccygeal, para/retrovesical, transvesical, and laparoscopic, have been described, but no consensus on the best method has been established. While complications are expected in all techniques, the transvesical and laparoscopic approaches are preferred due to lower risks of impotence, blood loss, and rectal injury [5].
Schwannomas are firm, grey masses that may show hemorrhage and cystic or xanthomatous changes on gross examination. Microscopically, the tumor is composed of different cellular densities with more cellular areas (Antoni A) consisting of spindled and oval nuclei, and less cellular areas (Antoni B) composed of loose, edematous and mucinous stroma. Verocay bodies, which are parallel columns of elongated nuclei on either side of acellular material, may also be present. Positive immunohistochemical reactions include S-100, Calretinin, CD56, SOX10, podoplanin, CD34, laminin, and vimentin, while negative reactions include Keratin, Neurofilament, Desmin, SMA, and EMA [5].
There is no known association between SLE and seminal vesicle tumors, but SLE or immunosuppression may be a risk factor due to the rarity of the disease and lack of known etiological factors. A larger cohort is needed to evaluate the same.
Conclusion
Primary seminal vesicle schwannoma is a sporadic tumor, and a preoperative histopathological diagnosis is necessary for optimal management. Minimally invasive surgical resection is the curative treatment, with proper preoperative counselling regarding potential complications such as impotence, blood loss, and rectal injury. Asymptomatic patients with schwannoma of the seminal vesicle can be monitored with regular followup.
Declarations
Acknowledgments: The patient in this case report was informed for the publishing of case details and accompanying images.
Funding: No financial implications as the patient was managed at a govt hospital.
Conflicts of Interest/competing interests: Authors have no conflict of interest.
Ethics approval (Include appropriate approvals or waivers): Ethical committee approval not required.
Consent to participate: Written informed consent was obtained from the patient.
Consent for publication: Patient has been informed about publication of his case in a scientific journal for educational purpose.
References
- Sato Y, Ohta S, Yamada Y, et al. Primary schwannoma of the seminal vesicle: a case report and literature review. Urol Case Rep. 2021; 36: 101599. doi:10.1016/j.eucr.2021.101599
- Huang, J., Cheng, Z., Li, R., Yao, N., Cao, J., Deng, S., & Wu, R. (2018). Pelvic mass: Schwannoma of the left seminal vesicle. Andrologia, 50.
- Belakhoua SM, Rodriguez FJ. Diagnostic Pathology of Tumors of Peripheral Nerve. Neurosurgery. 2021; 88(3): 443-456.
- Zhang, Y., Zhao, J., Xu, P., & Qi, Q. (2020). Multiple schwannoma of the seminal vesicle : a case report. Medicine. 2020; 99: 33(e21603).
- Furtado R, Tavora F, Epstein JI. Primary schwannoma of the seminal vesicle: a clinicopathologic series of 6 cases. Hum Pathol. 2016; 54: 33-38. doi:10.1016/j.humpath.2016.02.011.