
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Flail chest in posterior segment
Yudhyavir Singh1*; Baby Pegu1; Kapil Dev Soni2
1Department of Anesthesiology, Critical Care and Pain Medicine, AIIMS, New Delhi 110029, India.
2Critical and Intensive Care, JPNATC, AIIMS, New Delhi 110029, India.
*Corresponding Author : Yudhyavir Singh
Assistant Professor, Room No- 322A, JPNATC, Department of Anaesthesia, Critical and Pain Medicine, JPNATC, AIIMS, New Delhi 110029, India.
Tel: 9811140057;
Email: yudhyavir@gmail.com
Received : Nov 29, 2023
Accepted : Dec 26, 2023
Published : Jan 02, 2024
Archived : www.jcimcr.org
Copyright : © Singh Y (2024).
Citation: Singh Y, Pegu B, Soni K. Flail chest in posterior segment. J Clin Images Med Case Rep. 2024; 5(1): 2771.
Description
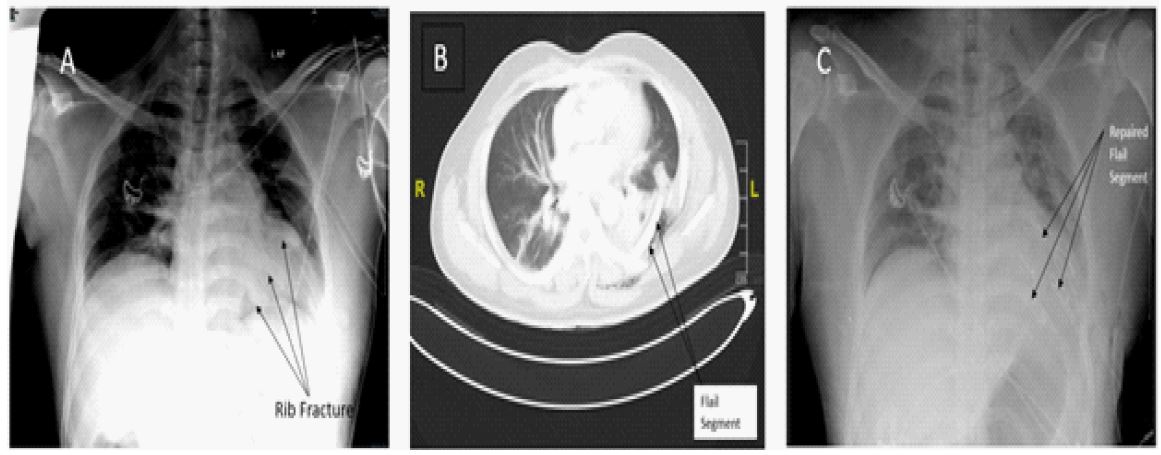
A 35-year-old male reported to the emergency department after a road traffic accident with complaints of chest pain on the left side and breathing difficulty. On the primary survey, his GCS was full, his airway was patent, breathing spontaneously with a respiratory rate of 28/min with paradoxical movement on the left of the chest, heart rate of 102/min, and blood pressure of 116/78 mmHg. On further evaluation, the chest compression test was positive on the left side, but FAST and eFAST scan were negative. Chest X ray showed 6th & 7th rib fractures on the left side posteriorly (Figure 1A). CT chest showed two-point fracture (flail segment) of left 6th, 7th & 8th rib posteriorly with displacement, single point fracture of 9th rib left minimal pneumothorax and moderate hemothorax with collapse left lower lobe (Figure 1B). The flail segment was abutting the left hemidiaphragm and mediastinum. Immediately the Intercostal drainage tube was placed on the left side. He required minimum oxygen support with facemask (4 litre/min) and shifted to the trauma intensive care unit for further management [1-3]. Pain was controlled with paracetamol and fentanyl infusion. For rib fixation of the flail segment, a posterolateral thoracotomy was done (Figure 1C). Intraoperatively, the findings of rib fracture were the same as seen in CT. The erector spinae block was put in for pain relief postoperatively. The indication of rib fixation is a must in ≥5 rib flail chest requiring mechanical ventilation or severe displacement found but can be considered in ≥3 flail ribs not requiring mechanical ventilation [4]. A posterior flail chest is very rare, indicating high-impact injury. The patient was shifted to the ward on day 2 and was discharged subsequently on day 7 uneventfully.
References
- Perera TB, King KC. Flail Chest. [Updated 2023 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534090/
- Dehghan N, de Mestral C, McKee MD, Schemitsch EH, Nathens A. Flail chest injuries: a review of outcomes and treatment practices from the National Trauma Data Bank. J Trauma Acute Care Surg. 2014; 76(2): 462-8.
- Alanwer, K.M., Refat, A.M. & Negm, E.M. Impact of flail chest injury on morbidity and outcome: ten years’ experience at a tertiary care hospital in a developing country. BMC Anesthesiol. 2023; 23: 229.
- Sawyer E, Wullschleger M, Muller N, Muller M. Surgical Rib Fixation of Multiple Rib Fractures and Flail Chest: A Systematic Review and Meta-analysis. J Surg Res. 2022; 276: 221-234.