
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Neonatal suppurative parotitis: Case report and review of literature
Malika El Omri*; Safa Jemli; Mouna Bellakhdher; Wassim Kermani; Mohamed Abdelkefi
Department of Otorhinolaryngology, Head and Neck Surgery, Farhat Hached Hospital, University of Sousse, Sousse, Tunisia.
*Corresponding Author : Malika El Omri, MD
Department of Otorhinolaryngology, Head and Neck Surgery, Farhat Hached Hospital, University of Sousse, Sousse, Tunisia.
Tel: +21656043690
Email: omri.malika6@gmail.com
Received : Nov 30, 2023
Accepted : Dec 27, 2023
Published : Jan 03, 2024
Archived : www.jcimcr.org
Copyright : © El Omri M (2024).
Abstract
Background: Neonatal suppurative parotitis is a rare entity, its diagnosis is essentially clinical with a good prognosis usually.
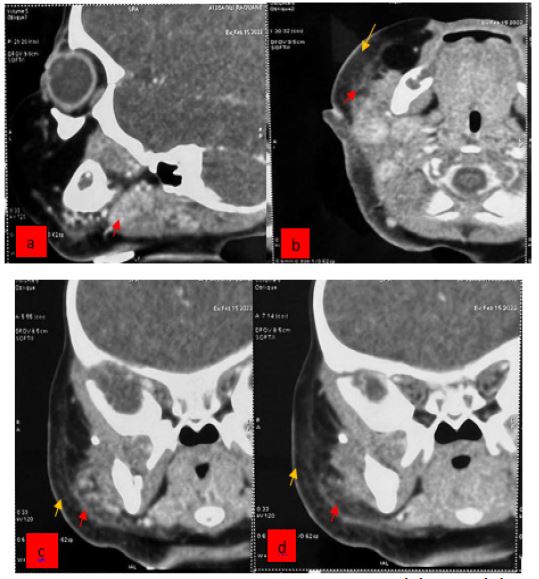
Case presentation: We report a case of a 21-day-old female whose been taken care of in our department for neonatal suppurative parotitis presenting with feverish, hard, red, tender swelling of the parotid loge. The swelling displaced the right earlobe outward and associated with purulent exudate from Stenson’s duct. A cervical and cerebral Computed Tomography scan showed a swollen right parotid gland of heterogeneous density and enhancement without detectable collection. The patient received intravenous antibiotherapy with a favorable evolution within 48 hours and no need for surgical treatment was found.
The aim of our work is to emphasize the diagnostic and therapeutic aspects of this clinical entity.
Conclusion: Practitioner should suspect suppurative parotitis in newborns presenting with an erythematous pre-auricular mass with or without any predisposing factors. The evolution is usually favorable and complications are rare with rapid and appropriate medical treatment.
Keywords: Neonatal; Acute suppurative parotitis; Sialadenitis; Treatment.
Citation: El Omri M, Jemli S, Bellakhdher M, Kermani W, Abdelkefi M. Neonatal suppurative parotitis: Case report and review of literature. J Clin Images Med Case Rep. 2024; 5(1): 2773.
Introduction
Parotitis is defined as an infection or inflammatory state of the parotid gland, which can be bacterial, viral, chronic, or recurrent [1]. While it is frequently seen in adults, suppurative acute parotitis is a rare condition in children, or even exceptional in newborns, Isolated case reports and small case series describe neonatal suppurative parotitis in neonates (NSP), but there is a paucity of information about predisposing factors for this entity [2]. We report a case of neonatal suppurative parotitis in a newborn taken care of in our department.
The aim of our work is to emphasize the diagnostic and therapeutic aspects of this clinical entity.
Case report
21-day-old female presented to ouremergency with a 2-day history of irritability, decreased oral intake, and preauricular swelling, all in a feverish context. She is the result of an uneventful pregnancy followed by vaginal delivery at term spontaneously with no complications or intrapartum trauma. At home, she was breastfeed well and eliminating normally. Two days before admission, the mother noted the acute onset of irritability while feeding and her time at the breast decreased followed by the swelling in front of his right ear increasing rapidly in size associated with local inflammatory signs. At the interrogation, the parents report no history of trauma to the infant’s face or head, the mother did not report any history of breast tenderness, recent skin infections, and she denied taking any medications or giving medications to the patient. On physical examination, the new born was feverish at 38,9. She was alert, nontoxic appearing and well hydrated. Cerviofacial examination found a swelling in front of the infant’s right ear, extending to the area underneath the ear lobe, over the angle of the mandible. The swelling displaced the right earlobe outward. The swelling was hard, redand tender. When crying, purulent exudate was found draining from Stenson’s duct. The rest of the physical examination was normal. Laboratory results were as follows: PCR count was 250. A spinal tap was performed; results were normal. Purulent material from Stenson’s duct; and cerebrospinal fluid, blood and urine samples were sent for culture. A cervical and cerebral Computed Tomography (CT) scan were performed showing a swollen right parotid gland of heterogeneous density and enhancement without detectable collection with significant infiltration of the right parotid and masticator spaces. The findings were consistent with acute suppurative parotitis. The newborn underwent intravenous antibiotic therapy with ceftriaxon (100 mg/kg/d) and gentamycin (3 mg/kg/d). 48 hours after admission, the newborn was clinically improved. The swelling had decreased and the overlying skin was less erythematous. The culture of the purulent material expressed from his parotid gland grew Staphylococcus aureus multisensible. The other cultures grew no pathogens and the newborn was discharged on oral cefpodoxime to complete 10 days of therapy. Follow-up examination 2 weeks later showed her to be in good health and his parotid swelling had completed resolved.


Discussion
Salivary gland infections are rarely observed in neonate, however, the parotid gland is the preferred site for this infection due to its exclusively production of serous secretions without the bacteriostatic properties of the mucoid component, typical of the submandibular gland that has a mixed sierous and mucous secretion containing IgA and lysozyme [2-4]. Despite this frequency, neonatal suppurative parotitis is characterized by a prevalence of 3.6-14/10 000 admissions [4,6]. In a review of the literature, only 32 cases of neonatal bacterial parotitis had been described over a period of 35 years [5]. It is characterized by a male predominance with a sex ratio of 3:1 [5]. Several risk factors have been identified in the literature as predictors of infant parotitis. It occurs more frequently in male sex infants, prematurity, dehydration, low birth weight, malnutrition, orogastric tube feeding and duct stasis [3,6]. Prematurity, considered as a major risk factor, usually due to prolonged hospitalization associated with procedures such as the use of an orogastric tube or a catheter, nasopharyngeal and endobuccal aspiration which can induce trauma to the oral mucosa and Stenon’s canal [7]. These traumas could thus favor an ascending infection from the oral cavity [8], without forgetting the higher risk of dehydration inducing a reduced salivary secretion and in saliva clearance [9,10].
Several mechanisms may be involved in NSP. First, it can occur by a retrograde way into the gland through decrease in saliva production and stasis, dilatation of the ducts (sialectasis) through scarring or obstruction by a stone or mass and congenital variations in ductal structure [2]. It can occur via the hemategenous route [10] or by transmission of bacteria during breastfeeding or through contaminated formula can be a potential [4,9]. Todoroki et al. described a case of neonatal suppurative parotitis in which stasis was probably due to congenital cytomegalovirus infection and maternal methyldopa treatment [10].
The diagnosis is essentially clinical, it is based on the association of a set of clinical signs, such as: fever, localized swelling, erythema, local warmth and painful tenderness of the parotid gland beginning between 7 and 14 days of life, purulent drainage from Stenson’s duct is pathognomonic but inconstant [1,2,6]. NSP is most often unilateral, bilateral is extremely rare [5].
The differential diagnosis arises with maxillary infections, trauma, lymphangiomas, hemangiomas, lipomasand adenomas [2,9].
The germs responsible for infectious parotitis are saprophytic germs of the oral cavity but also germs responsible for invasive infections [6]. The most common pathogen often implicated is Staphylococcus aureus. Less common isolates were other Gram-positive cocci (eg: viridians streptococci, Streptococcus pyogenes, Peptostreptococcus spp and coagulase-negative Staphylococcus spp), Gram-negative bacilli are, however, implicated more often in nosocomial and hematogenous infections secondary to sepsis (Klebsiella pneumonia, Escherichia coli, and Moraxella catarrhalis) and rarely anaerobic bacteria [3].
‘Multi-R’ resistant strains have been isolated in recent observations [10]. Only a few observations of suppurative parotitis due to Streptococcus agalactiae (group B streptococcus) have been reported, whereas this germ is responsible for 25 to 40% of infections of the newborn [6].
Parotid ultrasound allows highlighting a sialolith or parotid abscess, and if the patient shows no improvement after 48 hours, further imaging studies to rule out abscess formation or tracking of the infection into retropharyngeal areas should be conducted [2]. It reveals hypoechogenicity with heterogeneous areas within the gland. Parotid ultrasound is the examination to be preferred, especially in children, because it is rapid and non-invasive. It may also eliminate a differential diagnosis such as a cyst or another tumor-like mass [6]. CT and magnetic resonance imaging (MRI) are better performing for adults. The CT was performed for our case, in front of the redness of the pavilion and the associated retroauricular region raising suspicion of associated mastoiditis.
Some complications may occur such fistula formation, facial nerve palsies, mediastinitisand extension to the auditory canal are rare since the introduction of antibiotics [2].
Therapeutic management is essentially medical. It includes the correction of a possible dehydration and an immediate intravenous antibiotic therapy, a penicillinase resistant penicillin or first generation cephalosporin to effectively cover S. aureus along with clindamycin or a similar medication to cover possible anaerobic infection are good initial choices until better direction can be obtained from study of cultures of expressed material from Stenson’s duct [4,6]. The pressure of methicillin-resistant staphylococci may require the use of vancomycin. An adequate coverage for anaerobic, as well as aerobic, bacteria is provided with clindamycin, cefoxitin, imipenem or the comcombination of metronidazole and a macrolide or a penicillin plus beta-lactamase inhibitor [4].
Surgical drainage is reserved for complicated forms of an abscess or in the absence of clinical improvement after 24 to 48 hours of medical treatment [5,9].
The duration of antibiotic therapy is not precisely defined but a treatment of 7 to 10 days is essential until local inflammatory signs disappear. It is prolonged in premature infants, in the event of failure of other organs or when an anaerobic germ has been isolated [10]. Our case had a favorable evolution within 48 hours of intravenous antibiotic and no need for surgical treatment was found.
Conclusion
Although NSP is rare, practitioner should suspect suppurative parotitis in newborns presenting with an erythematous pre-auricular mass with or without any predisposing factors.
Declarations
Consent: Informed consent was obtained from the parents of our patient.
Disclosures: The authors have nothing to disclose.
Competing interests: The authors declare no competing interests.
References
- Stong BC, Sipp JA, Sobol SE. Pediatric parotitis: A 5-year review at a tertiary care pediatric institution. International Journal of Pediatric Otorhinolaryngology. 2006; 70(3): 541‑4.
- Schwab J, Baroody F. Neonatal Suppurative Parotitis: A Case Report. Clin Pediatr(Phila). 2003; 42(6): 565‑6.
- Sabatino G, Verrotti A, de Martino M, et al. Neonatal suppu- rative parotitis: a study of five cases. Eur J Pediatr. 1999; 158: 312-4.
- Decembrino L, Ruffinazzi G, Russo F, Manzoni P, Stronati M. Monolateral suppurative parotitis in a neonate and review of literature. International Journal of PediatricOtorhinolaryngology. 2012; 76(7): 930‑3.
- Spiegel R, Miron D, Sakran W, Horovitz Y. Acute neonatal suppurative parotitis: case reports and review: The Pediatric Infectious Disease Journal. 2004; 23(1): 76‑8.
- Makhoul J, Lorrot M, Teissier N, Delacroix G, Doit C, Bingen E, et al. Parotidite bactérienne aiguë chez les nourrissons de moins de 3mois : étude rétrospective dans un centre hospitalier universitaire. Archives de Pédiatrie. 2011; 18(12): 1284‑9.
- Chevalier J, Jadcherla SR. Parotid swelling in a premature neonate. Am J Perinatol. 2002; 19: 435-7.
- Fathalla B, Collins D, Ezhuthachan S. Acute suppurative parotitis: uncommon presentation in a premature infant. J Perinatol. 2000; 1: 57-9.
- Özdemir H, Karbuz A, Çiftçi E, Fitöz S, İnce E, Doğru Ü. Acute neonatal suppurative parotitis: a case report and review of the literature. International Journal of Infectious Diseases. 2011; 15(7): e500‑2.
- Isfaoun Z, Radouani MA, Azzaoui S, Knouni H, Aguenaou H, Barkat A. Parotidite aigue néonatale suppurative: à propos de trois cas cliniques avec revue de la littérature. Pan Afr Med J. 2016; 24: 286.