
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 5
Management and clinical features of extranodal tuberculosis: About 7 cases
Malika El Omri*; Safa Jemli; Mouna Bellakhdher; Wassim Kermani; Mohamed Abdelkefi
Department of Otorhinolaryngology, Head and Neck Surgery, Farhat Hached Hospital, University of Sousse, Sousse, Tunisia.
*Corresponding Author : Malika El Omri
Department of Otorhinolaryngology, Head and Neck Surgery, Farhat Hached Hospital, University of Sousse, Sousse, Tunisia.
Tel: +21656043690;
Email: omri.malika6@gmail.com
Received : Nov 30, 2023
Accepted : Dec 27, 2023
Published : Jan 03, 2024
Archived : www.jcimcr.org
Copyright : © El Omri M (2024).
Abstract
Background: Extranodal tuberculosis is a rare pathology in ear nose and throat (ENT) sphere. It remains a worldwide health problem despite the development seen.
Results: We report 7 cases of extranodal localizations, collected at the ENT department of Farhat Hached Hospital Sousse, between 2008 and 2022.
There were 2 women and 5 men, aged between 15 and 45 years (average: 29 years). The disease affected the cavum in 2 cases, the parotid gland in one case, the palatine tonsils in 2 cases the pharyngo larynx in one caseand a retropharyngeal space in one patient. The diagnosis was histopathological in all cases. All our patients received anti-tuberculosis treatment. The evolution was favorable in all cases.
Conclusion: Practicians should keep in mind the involvement of the ENT sphere during tuberculosis in endemic areas and confirm it by bacteriological and histological examinations. The treatment is based on anti-tuberculosis drugs.
Keywords: Tuberculosis; ENT sphere; Extranodal.
Citation: El Omri M, Jemli S, Bellakhdher B, Kermani W, Abdelkefi M. Management and clinical features of extranodal tuberculosis: About 7 cases. J Clin Images Med Case Rep. 2024; 5(1): 2774.
Introduction
Tuberculosis remains a major public health problem as well as a major cause of morbidity and mortality in the global population. Approximately one-third of the world’s population has latent infection with Mycobacterium tuberculosis [1]. Tunisia represents the third country in the world to be endemic to Tuberculosis, extrapulmonary tuberculosis represents 15% but extranodal Head and neck localization are very rare [2]. The aim of our work is to note the epidemiological, clinicaland therapeutic particularities of this location of tuberculosis.
Materials and methods
This is a retrospective study covering seven cases of extra-nodal tuberculosis, collected at the ENT department of Farhat Hached Hospital in Sousse, over a period of 14 years [2008-2022].
For each patient, a complete clinical examination was carried out, including a questioning (age, sex, medical history, concept of contagion, functional sign...) and a physical examination specifying the semiological characteristics according to location as well as the presence of possible cervical lymphadenopathy. Certain additional examinations were requested systematic way: a blood count, erythrocyte sedimentation rate (ESR), intradermal tuberculin reaction (IDR), and chest x-ray. A contrast-enhanced computed tomography (CT) scan was done in retropharyngeal tuberculosis. Magnetic resonance imaging (MRI) was done on parotid tuberculosis. Chest X ray of the lungs was done in all cases. The diagnosis of extranodal tuberculosis was based on pathological findings of the biopsy specimen collected from the different locations of tubercular after with highlighting a granulomatous infiltrate with or without necrosis caseous. No fine needle aspiration cytology (FNAC) was done. Clinical signs in addition to the recovery under anti-tuberculosis treatment reinforced the positive diagnosis of tuberculosis.
Results
There were 5 male and 2 female patients aged from 15 to 45 years, with a mean age of 29 years. The disease affecting the locations in the head and neck region was 2 in the tonsils, 3 in the nasopharynx, one in the pharyngolarynx, one in the parotid gland, and one in the retropharyngeal space. Two cases had a family history of tuberculosis. The mean duration of symptoms was 2 months. Clinical presentations were varied as per site of involvement (Table 1); in nasopharyngeal tuberculosis, thepatient consulted for unilateral epistaxis assoicated to an ipsilateral nasal obstruction, the diagnostic nasal endoscopy showed bulged and irregular mucosa at the posterosuperior part of the nasopharynx in both cases. Patients of pharyngolaryngeal tuberculosis presented with chronic dysphonia and dysphagia and ulcerative lesion over the vocal cords. Parotid tuberculosis presented with a parotid swelling where the examination confirmed a mass firm swelling, attached to the underlying tissue, with no skin inflammation nor facial weakness. One patient ofcervical Pott’s disease revealed by a retropharyngeal abscess presented a febrile anterior displacement of the posterior pharyngeal wall with overlying congested mucosa, with no imminent airway compromise. There was no trismus. A bilateral palpable tender upper neck swelling of about 5 cm was found. The palpation of the cervical spine was very painful. Routine blood investigations such as total white cell count and differential count found biological inflammatory syndromein five cases. Tuberculin test was done in all cases and positive in the 7 cases. Ultrasound of the neck was done in one case of parotid tuberculosis showing a cystic mass of the right parotid gland. A contrast-enhanced computed tomography (CT) scan was done in the case of tuberculous retropharyngeal abscesses demonstrating a ring-enhancing lesion in the retropharyngeal space at the level of C3 suggestive of a retropharyngeal abcess (RPA) associated with marked erosion of the anteriorarch of the third and the seventh cervical vertebrae (Figure 1). Only one patient underwent an MRI (parotid tuberculosis) revealing a cysticlikelesion extended in the deep parotid gland. The lesion had a low signal on T1- weighted image, and high signal on T2- weighted image associated with inflammatory lymph nodes (Figure 2).
Biopsy and histopathological examinations were done in all of our cases. One patient had undergone superficial parotidectomy. The drainage of the RPA was performed through an intraoral vertical incision in the posterior pharyngeal wall. Histopathology report confirmed tuberculosis in all the cases by demonstrating epithelioid granuloma with or without caseating necrosis. A complete pre-therapeutic assessment was carried out in all patients. All the cases received antitubercular treatment. Four drugs such as rifampicin, isoniazid, ethambutol, and pyrazinamide were given in the intensive phase for 2 months followed by isoniazid and rifampicin in a continuation phase for 6-8 months. All patients had favorable outcomes (Figure 3) and no one had recurrence.
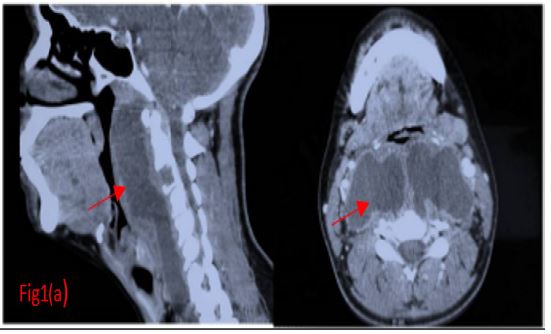
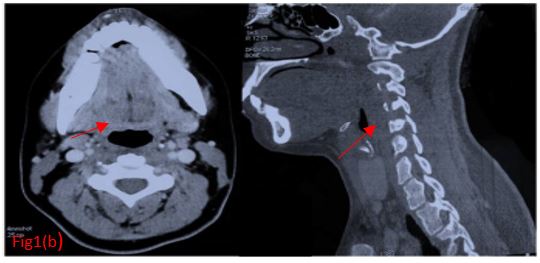
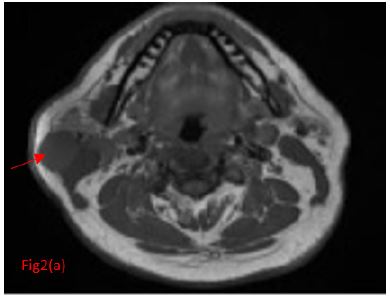
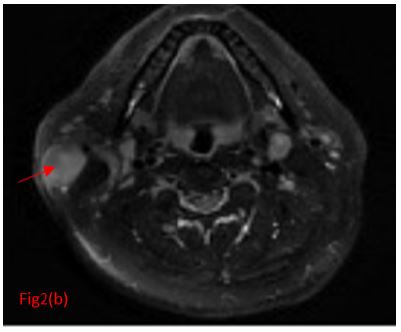

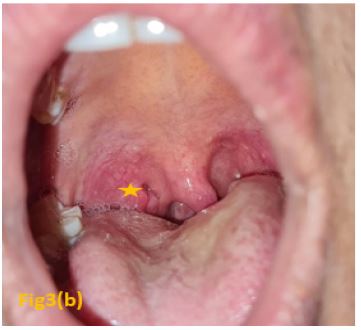

Table 1: Clinical presentations per site of involvement.
| Localization | Nasopharynx(2 cases) | Tonsillar palatine (2cases) | Parotide (1case) | Pharyngolarynx(1 case) | Retropharyngeal abcess(Pott’s disease,1case) |
|---|---|---|---|---|---|
| Functionnal Signs | Epistaxis* 2 | Odynophagia,dysphagia high dysphagia | Cervicalswelling | Highdysphagia | Dysphagia |
| Physicalexamination | Bulged and irregular mucosa at the posterosuperior part*2 | Indurated right palatine tonsil (2 cases) | Firm parotidswelling | Ulceration at the level of the right epiglottic ary fold as well as atthe level of the lateral and medial wall of the pyriform sinus | Asymmetrical bulging of the posterior wall of the oropharynx |
| Biological inflammatory syndrome | - | + | + | + | + |
| TuberculinIDR | + | + | + | + | + |
| Testing for tuberculosis in sputum | - | - | - | + | - |
Discussion
Tuberculosis is an infectious disease that still represents a public health problem. Until the Coronavirus (COVID-19) pandemic, tuberculosis was the leading cause of death from an infectious agent, ranking before HIV/AIDS [1]. Its overall incidence observed a reduction of 11% between 2015 and 2020, with an incidence rate at the national level varying from less than 5 to more than 500 new cases per 100,000 inhabitants per year [3]. Pulmonary tuberculosis is the most common presentation found in 60 to 70% of cases [4,5]. The extrapulmonary localization, found in 20 to 30% of cases, is dominated by the lymph node localization observed in 10% of cases [4]. However, head and neck extranodal localization of tuberculosis is very rare observed in almost 1,8% [6].
Several routes of dissemination to ENT sites have been defined [7];
• The hematogenous route most often from a pulmonary site.
• The lymphatic route due to a locoregional mucocutaneous involvement.
• The ductal route through the bronchial sputum containing the bacilli is also called upward diffusion.
• The direct route from the external environment, this mechanism explains rare primitive forms.
These inoculation mechanisms explain the topographical variety of lesions and the possibility of multiple location shapes.
Nasopharyngeal tuberculosisis the most common according to literature [7]. It is mainly observed in young male subjects, no linear presentation is specific and it often takes on a pseudotumoral appearance [8], clinical signs are similar to nasopharyngeal carcinoma [9]. Otological, rhinological signs or cervical lymphadenopathy are most often observed, unilaterality is often the rule [8]. Our patients presented both unilateral epistaxisassociatedwithhypoacusis in one case. The most common endoscopic appearance is a budding formation mainly posterior superior as observed in our patients.
Tonsillar tuberculosis is an exceptional entity because of the antiseptic action of saliva and innate resistance of tonsils to mycobacterium tuberculosis [10,11]. Clinically, it presents as tonsillar enlargement, sore throat, dysphagia, odynophagia, painful ulceration, white patches associated or not with cervical lymphadenopathy [12]. Our patient presented odynophagia, high dysphagia, an indurated tonsil increased in size associated with a magma of ipsilateral adenopathy in a single case.
Tuberculosis of the salivary gland is more often associated to a pulmonary tuberculosis than a primary extrapulmonary tuberculosis [13]. The parotid gland presents 70% of salivary glands tuberculosis [14]. Santosh Kumar Swain have found one case among 12 extranodal tuberculosis equivalent to 8% [15]. It can appear as a nodular or diffuse form, with an acute or chronic onset with no specific symptoms [14]. MRI, CT and cervical ultrasound are not specific for parotid tuberculosis and suggest malignancy in most cases [14]. The presence of necrosis in tuberculosis reduces the contribution of FNAC, however incisional biopsy is contraindicated because of the cutaneous fistula formation which is difficult to heal [14].
Primary pharyngo-laryngeal tuberculosis is extremely rare even in endemic area [12]. It is more often seen as a dissemination of a pulmonary tuberculosis found in 15 to 37% of cases of pulmonary tuberculosis, nut rarely as a primitive one [15]. It is observed in two peaks, at 30 and 60; our patient had 32 years old. Diagnosis confirmation requires direct sputum microscopy, molecular biology techniques and/or histological analysis. Imaging investigation has a valuable contribution to precise the sites of involvement, pattern and extension of the disease. It can endanger the vital prognosis in the face of possible obstruction of the upper airway, despite preservation of the architecture of the pharyngolarynx [10].
Tuberculosis involvement of the retropharyngeal space is exceptional [15], usually due to spinal tuberculosis [15]. The tuberculosis infection extends through intervertebral disks to multiple vertebrae and soft tissues, thus forming an abcess [3]. Symptoms are not specific. The diagnosis is based on radiological and bacteriological assessment. Treatment implicates a multidisciplinary team, first the evacuation of the collection, then anti-tuberculosis chemotherapy [3].
Other tuberculosis locations have been described in Literature:
- Thyroid tuberculosis, is seen in 0,5% to 1,15% of tuberculosis of head and neck, isoften secondary to a hematogenous dissemination of the germ.
- Nasosinus tuberculosis remains however, a rare entity estimated at 1% of tuberculosis of head and neck. The cartilaginous portion of the nasal septum and the turbinates are the most interested sites [7].
- Auricular tuberculosis remains also a rare entity, representing 0.4% of otitis media according to Awan 1983 [6], the last case was described by Santosh Kumar Swain et al in 2020. The diagnostic difficulty lies in the fact that it presents itself like other suppurative otitis media [7].
The intradermal action of tuberculin is not always positive [7]. All our patients benefited from it and it was positive in all cases. The certainty of tuberculosis in ENT all sites is histological and/or bacteriological [6]. However, histology can provide formal proof within a reasonable time, unlike bacteriology whose result (culture) canrequire several months. In fact, it reveals the presence of epithelial-gigantocellular foci with caseal necrosis PCR test is not a usual exam, it is often asked in case of strong clinician suspicion of tuberculosis with negative cultures [2]. Diagnostic confirmation was histological in all our patientsand the biopsy proved sufficient for the positive diagnosis in most of the cases collected, thus avoiding us having to wait the result of the culture and allowing us to start the treatment.
As per the world Health Organization (WHO) guidelines, extrapulmonary tuberculosis should be treated by four drug regimen in the first 2 months followed by two drugs for the next 4 months, is mainly based on isoniazid, rifampicin, pyrazinamide and streptomycin currently replaced by ethambutol [1]. Mainly extrapulmonary tuberculosis is treated medically, surgery is usually necessary in order to establish the positive diagnosis and initiate treatment [15]. Al our patients received anti tuberculosis treatment following the diagram described in the guidelines.
Conclusion
Extranodal tuberculosis of the ENT sphere is a rare pathology. Clinically it poses diagnostic difficulties with neoplastic pathology. The diagnosis is essentially histopathological. Treatment is based on anti-tuberculosis drugs and the evolution is generally favorable.
Declarations
Consent: Informed consent was obtained from all the patient.
Disclosures: The authors have nothing to disclose.
Competing interests: The authors declare no competing interests.
Funding: No funding or sponsorship was received for this study or publication of this article.
References
- World Health Organization. Shaping the global innovation and access landscape for better paediatric medicines. Geneva: World Health Organization; 2022.
- Mezri S, Sayhi S, Amira MBet al. Coexistence of Tuberculosis and Metastatic Undifferentiated Carcinoma of Nasopharynx in Cervical Lymph Node. Otolaryngology – Open Journal. 2019; 5: 26-28.ssss
- Global tuberculosis report 2020. Geneva: World Health Organization; 2020.
- Yombi JC, Olinga M, Ubald. La tuberculose : épidémiologie, aspect clinique et traitement.Louvain médical. 2015; 134(10): 549-9.
- Ossalé Abacka KB, Koné A, Akoli Ekoya O, Bopaka RG, Lankoandé Siri H, Horo K. Tuberculose extrapulmonaire versus tuberculose pulmonaire : aspects épidémiologiques, diagnostiques et évolutifs. Revue de Pneumologie Clinique. 2018; 74: 452–7.
- Touati MM, Darouassi Y, Chihani M, Lakouichmi M, Tourabi K, Ammar H, et al. La tuberculose extra-ganglionnaire primitive de la sphère ORL: à propos de 15 cas. Pan Afr Med J. 2014; 19(179): 1-6.
- Gassab E, Kedous S, Berkaoui A, Sayeh N, Harrathi K, Koubaa J, et al. Tuberculose extra ganglionnaire de la tête et du cou. Journal Tunisien d’ORL et de Chirurgie Cervico-Faciale. 2011; 24: 26-30.
- Hadid F, Oulghoul O, Benjelloun H, Benhommad O, Raji A, Rochdi Y. Nasopharngeal Tuberculosis Simulating Cancer: About 2 Cases. EJMED. 2021; 3: 46-8.
- Adnane C, Adouly T, Oubahmane T, Rouadi S, Abada R, Mahtar M, et al. Tuberculose nasopharyngée : à propos de 3 cas. Annales françaises d’Oto-rhino-laryngologie et de Pathologie Cervico-faciale. 2014; 131(4): A129.
- Sellami M, Mnejja M, Charfi S, Ghorbel A. Tuberculosis of the tonsil simulating a cancer. The Lancet Infectious Diseases. 2017;17: 1317.
- Dhanasekar T, Inba Shyamala R, Arshad AM, Rajagopalan. An interesting case of tonsillar tuberculosis in a 10-year-old boy. Journal of Clinical Tuberculosis and Other Mycobacterial Diseases. 2020; 20: 100162.
- Das A, Das S, Pandit S, Basuthakur S. Tonsillar tuberculosis: a forgotten clinical entity. J Family Med Prim Care. 2015; 4: 124.
- Ali GM, Houda B, Zineb B, Sophia N, Razika B, Anas BM. Evolution of Parotidial Tuberculosis after Medical Treatment. 2021; 6: 130-133.
- Gupta V, Patankar K, Shinde A, Bhosale C, Tamhane A. Tuberculosis of the Parotid Gland. Case Reports in Radiology. 2012; 2012: 1-3.
- Swain S, Mohanty J, Sahu M. Extranodal tuberculosis of the head and neck: Our experiences at a tertiary care teaching hospital of East India. Med J DY Patil Vidyapeeth. 2020; 13: 465.