
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 5
Appropriateness of timing of initial antibiotic prescription in ICU and outcome
Debasmita Paul1; Mahua Bhattacharya2; Moumita Kundu3*
1Assistant Professor, Department of Pharmacology, Bharat Technology, Uluberia, Howrah, West Bengal 711316, India.
2AMRI Hospital, Kolkata, West Bengal 700099, India.
3Assistant Professor, Department of Pharmacy, Anand College of Education, Kabilpur, Debra, West Bengal 721126, India.
*Corresponding Author : Moumita Kundu
Assistant Professor (Department of Pharmacy) at Anand College of Education, Kabilpur, Debra, West Bengal 721126, India.
Email: moumitapharmacy22@gmail.com
Received : Nov 16, 2023
Accepted : Dec 27, 2023
Published : Jan 03, 2024
Archived : www.jcimcr.org
Copyright : © Kundu M (2024).
Abstract
Objectives: There is strong evidence that appropriate antibiotic medication is the cornerstone of effective severe sepsis, sepsis and septic shock treatment. It has been acknowledged that delaying the start of proper antibiotic medication increases the risk of death. This study was a single-centre retrospective observational study involving ICU patients to investigate the association between antibiotic treatment timing and survival.
Design: Retrospective chart review of every patient with severe sepsis, sepsis and septic shock admitted to ICU.
Setting: Every patient with severe sepsis, sepsis and septic shock was admitted to ICU of Advanced Medical Research Institute (AMRI), Dhakuria, Kolkata over the 10 months of observational single centre study. This hospital provides tertiary care with 20 ICU beds.
Patients: Two hundred eighty-four patients brought to the intensive care unit (ICU) with severe sepsis, sepsis and septic shock, from June 2013 to March 2014, was evaluated.
Measurements and main results: Following the diagnosis of sepsis, 284 individuals were given antibiotics and were included in the study. In-hospital mortality was 29.7% for the entire group. There was a significantly higher level of statistical significance in the risk of mortality linked with the number of hours between the start of the antibiotic dose and death. Regardless of the amount of organ failure, the results were identical in patients with severe sepsis and septic shock.
Conclusions: Examination of this specific patient group who had severe sepsis, sepsis and septic shock revealed that a delay in the delivery of the initial antibiotic was linked to a higher in-hospital mortality rate. Every hour that antibiotic distribution did not occur increased mortality risk. These findings highlight how critical it is to recognize and treat severe sepsis, sepsis and septic shock as soon as possible in the hospital setting.
Keywords: Severe sepsis; Sepsis and septic shock; Antimicrobial therapy; Timing; Antibiotic administration; Sepsis treatment; Hospital mortality rate.
Citation: Paul P, Bhattacharya M, Kundu M. Appropriateness of timing of initial antibiotic prescription in ICU and outcome. J Clin Images Med Case Rep. 2024; 5(1): 2775.
Introduction
Sepsis is characterized as Systemic Inflammatory Response Syndrome (SIRS) in the context of an infection, whether indicated or assumed. Features of SIRS Could be as well evident in conditions like acute severe pancreatitis, trauma and burn. Severe sepsis is that part of disease spectrum where there is sepsis induced at least two organs dysfunction acute respiratory distress and acute renal failure or cardiovascular dysfunction [1]. Septic shock is a life-threatening illness characterized by hypotension which is not responding to adequate fluid management, along with impaired organ function and/or failure. Septic shock can develop in patients infected with a variety of gram-positive and gram-negative bacteria, viruses, fungi, rickettsiae, spirochetes, protozoa, and parasites. The sepsis syndromes are a disease phase that evolves from sepsis (infection with an inflammatory response) to severe sepsis (organ malfunction) to septic shock (tissue hypoperfusion).
Severe sepsis and septic shock are medical emergencies which affect 18 million individuals per year world wide [2]. This rate may represent an underestimation on a global assessment, as some developing countries lack the advanced microbiology services necessary to quantify the devastation secondary to infection.
Sepsis is by definition a consequence of infection. Efforts to identify and manage the clinical site of infection and to establish the microbiology are of critical importance. While this appears to be self-evident, studies indicate a surprising frequency of inadequate or absent workup, and suboptimal or inappropriate antibiotic therapy [3]. In one large prospective trial of over 2,000 patients, antimicrobial therapy in which the offending bacterium is exposed was later shown to be resistant occurred in 32% of patients [4]. Mortality is reduced from 34% to 18% when appropriate antimicrobials are prescribed at the onset of sepsis [5].
The choice of antimicrobials is focused on the patient’s history and physical exam, data collection including imaging studies, Gram stain data, and a knowledge of local and regional resistance patterns and epidemiology. Select antibiotic with low resistance potential & good safety profile is very important. The primary sites of in sepsis and septic shock, however, remain either intra-abdominal (includes urinary) or pulmonary in over 90% of cases.
The optimum timing of application of antimicrobials remains nebulous. SCC guidelines suggest that an antimicrobial regimen should be started within one hour of a diagnosis of sepsis. There are, however, no published data that establish a crucial ‘time to antibiotic’ interval. SSC also recommends that antibiotics be re-evaluated after 48-72 hours to determine the adequacy of the antimicrobials and to when those drugs not required [6].
Rapid administration of appropriate antibiotics in correct doses plays a major role in patient survival [7]. In adults diagnosed with septic shock, efficient antimicrobial use in the first hour of recorded hypotension was linked with better outcome to hospital discharge. Regardless of an ongoing rise in death rates with increasing complications, only 50% of patients with septic shock acquired efficient antimicrobial treatment within 6 hrs of reported hypotension. Infections with gram-negative bacteria linked with septic shock greater than anything else, etiologic agent; therefore, antibiotic selection must include those drugs with superior gram-negative coverage. The selection of appropriate antibiotics should be based on sound clinical judgment plus knowledge of the antibiotics used. The principles of rational therapy include the following: (1) know the type of microorganisms or suspected organism being treated; (2) be familiar with resistant organisms in both the community as well as the hospital; and (3) initiate combination therapy with a beta-lactam antibiotic plus an aminoglycoside or use immunotherapy with either a carbapenem or selected third generation cephalosporin. After culture results are known, the antibiotic regimen should be narrowed to cover the specific infecting microorganism using the least expensive, least toxic antibiotic available.
The choice of antimicrobials for patients with severe sepsis, sepsis, or septic shock depends on various factors, including the suspected source of infection, local resistance patterns, and patient-specific factors. Here are some antibiotics frequently used for treating severe sepsis, sepsis and septic shock:
1. Broad-spectrum Beta-lactam Antibiotics:
Piperacillin-tazobactam; Ceftriaxone; Ceftazidime; Meropenem; Imipenem-cilastatin.
2. Glycopeptides:
Vancomycin; Teicoplanin.
3. Oxazolidinones:
Linezolid.
4. Aminoglycosides:
Gentamicin; Tobramycin; Amikacin.
5. Fluoroquinolones:
Ciprofloxacin; Levofloxacin.
6. Tetracyclines:
Doxycycline; Minocycline.
7. Clindamycin
8. Metronidazole
9. Antifungal Agents (if indicated):
Fluconazole; Amphotericin B; Caspofungin.
In the Intensive Care Unit department, we investigated the result of antibiotic scheduling on survival in patients with severe sepsis, sepsis and septic shock. We expected that earlier antimicrobial treatment administration in patients (within the time limit advised by the Surviving Sepsis Campaign) would be related to improved mortality. Nonetheless, these findings must be validated, and the most appropriate time of antibiotic delivery in sepsis patients remains unknown. As a result, this research aimed to look at the relationship between antibiotic administration timing and mortality to see if there was an ideal time window for intensive antibiotic therapy in patients with severe sepsis, sepsis and septic shock. We also wanted to examine the mortality rate in patient population of severe sepsis, sepsis and septic shock, who received appropriate antibiotics and inappropriate antibiotics therapy according to their blood culture reports.
Patient selection
• Inclusion cirteria:
All patients admitted in Intensive Care Unit and on antibiotic any moment throughout their stay in the Intensive Care Unit, was included.
• Exclusion cirteria:
Post operative patients after elective surgery who came for observation to Intensive Care Unit or patients who received antibiotics as routine prophylaxis were excluded.
Patients who received antibiotics, but discharged from Intensive Care Unit or hospital on a release bond (DORB) were excluded.
Study design
This was a single-center retrospective observational research including ICU patients.
Study setting and duration
We conducted a retrospective chart review of every patient with severe sepsis, sepsis and septic shock admitted to Intensive Care Unit of Advanced Medical Research Institute (AMRI), Dhakuria, Kolkata over the 10 months period observational research study between June 2013 to March 2014. The hospital has tertiary care status with 20 ICU beds.
Ethical approval
This study was approved by the institution’s research ethics board.
Methodology
Data was recorded on a standardized data collection form.
Clinical data: Data regarding the following details were obtained for each patient from medical records: Admission date in hospital & ICU, age, sex, co-morbidities present, admission diagnosis and APACHE IV score. It was noted that a number of comorbid conditions were present: Heart Failure, Diabetes Mellitus, Chronic Obstructive Pulmonary Disease (COPD), Hepatic Dysfunction, Renal failure, cerebrovascular accident, Heart Failure, Malignancy, Administration of immunosuppressive drugs, Chronic Kidney Disease (CKD). Patients categorized in SIRS, severe sepsis, sepsis and septic shock, according to 1991 Society of Critical Care Medicine/American College of Chest Physicians unanimity on what constitutes sepsis. According to the criteria, two of the following four requirements had to be met by case patients in addition to a recorded or suspected illness: (1) a respiratory rate of 20 breaths/min or Pco2 of 32 mm Hg; (2) a heart rate of 90 beats/min and (3) a WBC count of 4,000/L, 12,000/L, or 10% immature (bands) forms; (4) a core temperature of 36°C or 38°C. A shock condition defined as chronic hypotension needing pressor treatment. Also indicated was the infection’s origin.
Microbiological data: Microbiologic data collected from the culture report that sent for the patients, were noted including the results and date.
Treatment data: It was recorded when the first antibiotics were given following an ICU admission. The antibiotic’s dosage and delivery technique were recorded. If the patient was given an antibiotic as a first treatment and the cultured bacteria showed in vitro responsiveness to that antibiotic, then antibiotic delivery was deemed suitable. Antibiotics were deemed suitable in the event of negative cultures if they were administered in compliance with regional protocols and were broad spectrum medications.
Outcome data: Outcome data included intensive care unit and hospital mortality, so also the morbidity data, which included intensive care unit and hospital duration of stay and resolution of organ failure from time of antibiotic administration. Appropriate statistical test applied to analyze the data.
Statistical analysis
• Demographic variables were discussed using mean ± SD values.
• Patients’ mortality rate described in percentage and Odds ratio.
Odds ratio is a statistical parameter used for determining the significance of time axis on the mortality. Odds ratio represents odds of death with increase in delay of antibiotic administration and is calculated as below.
| Time Series | Expired | Survived | TotalPatients | %Mortality | OddsRatio |
|---|---|---|---|---|---|
| 0– 1 hr | X1 | Y1 | T1=X1+Y1 | (X1/T1)X100 | |
| 1– 2 hr | X2 | Y2 | T2=X2+Y2 | (X2/T2)X100 | OR |
Odds Ratio (OR) = (X2/Y2) / (X1/Y1)
Odds ratio greater than 1 signifies the increase in mortality with respect to delay in antibiotic administration represented by time series.
Results and data analysis
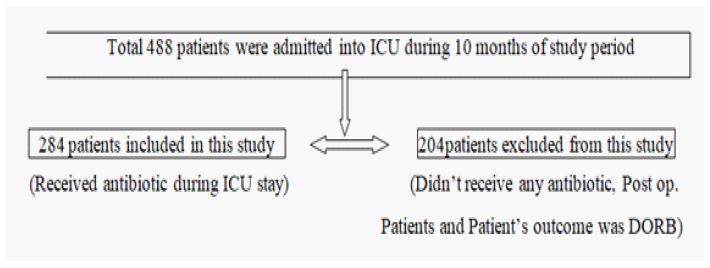
During this 10-month period observational single center study between June 2013 to March 2014, ICU admissions totaled 488 patients. 204 of them were removed because no antibiotics were given. Post operative patients after elective surgery who came for observation to ICU and patients who received antibiotics, but discharged from ICU or hospital on a release bond (DORB).
Total 284 patients were fit the inclusion criteria.
Demographic and descriptive data
The average age of patients was 63.45±16.69, with 54% males and 46% females. Average APACHE IV score determined from the most abnormal results within 24 hrs of infection was 49.24±18.74. The Patient population divided into No severe sepsis, sepsis and septic shock category, according to the severity of infections. Almost half of the patient population fell on sepsis category. The frequency of chronic co-morbidities among severe sepsis, sepsis and septic shock patients were noted, highest co morbid conditions are Hypertension (49%) and Diabetes Mellitus (35%). The frequency of clinically defined infection sites is listed. Renal (36%) and Chest (21%) are the mostly found source of infections resulting in sepsis, severe sepsis and septic shock patients. Patient’s characteristics and clinical data is displayed in Table 1.
Table 1: Patients characteristics and clinical data
| Variable | Mean ± SD or n (%)* |
|---|---|
| Age | 63.45± 16.69 |
| Sex (Female) | 132(46%) |
| Sex (male) | 152(54%) |
| Severity of illness | |
| APACHE** IV | 49.24± 18.74 |
| Comorbid conditions | |
| Diabetes mellitus | 95(35%) |
| Hypertension | 133(49%) |
| Chronic kidney disease | 35(13%) |
| Malignancy | 7(3%) |
| Source of infection | |
| BRAIN and MENINGES | 6(3%) |
| CHEST | 43(21%) |
| CARDIAC | 7(3%) |
| ABDOMEN | 15(7%) |
| RENAL | 75(36%) |
| UNKNOWN | 29(14%) |
| OTHERS | 33(16%) |
*Results expressed as mean ± SD or n (%)
**APACHE: acute physiology and chronic health evaluation
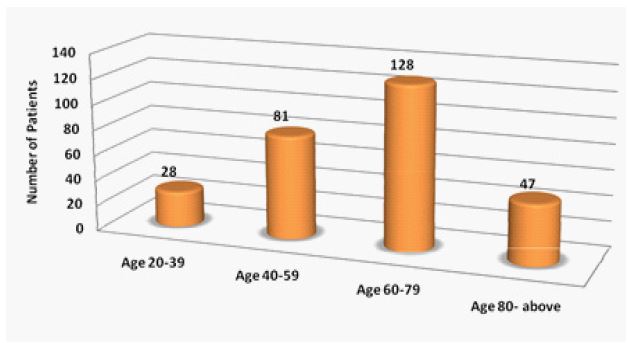
Patient’s age group distribution
The entire patient population is split up into four age categories. The majority of the patients were in the age group of 60-79 yrs (45%) and the lowest number patients were in the age group of 20-39 yrs (10%). Patient’s age groups distributions are described in Figure 1.
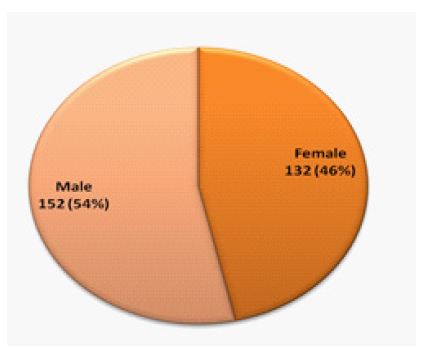
Gender ratio of patients
Among total patients, male patients were 152 (54%) and female patients 132 (46%). The male patient’s ratio was 8% higher than female patients.
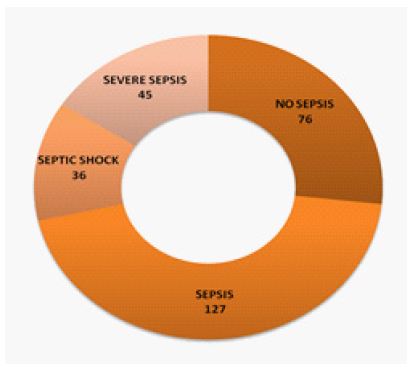
Sepsis spectrum of patients
Total 284 patients divided into four groups according to severity of infections. 127 patients had sepsis, 76 patients had no sepsis, 45 patients had severe sepsis and 36 patients had septic shock. The sepsis patient population is highest 45% and Septic shock patient population is lowest 12%. Sepsis spectrum of total patients is shown in Figure 3.
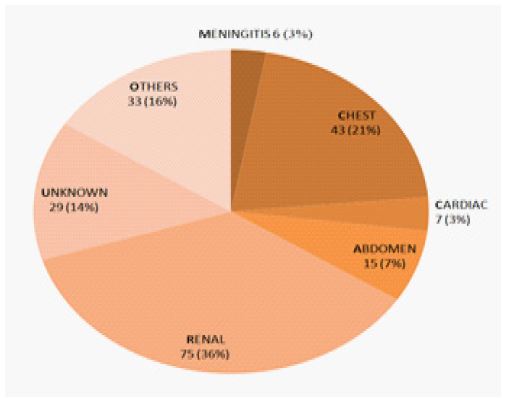
Source of sepsis infections
The sources of infections like meningitis, chest, cardiac, abdominal, renal, unknown and others were noted in severe sepsis, sepsis and septic shock patients. The major sources of infections are renal (mainly urinary tract infection), presented in 75(36%) patients, Chest, presented in 43(21%) patients, Abdomen, presented in 15(7%) patients; Cardiac, presented in 7(3%) patients; Meningitis presented in 6(3%) patients, unknown sources, presented in 29(14%) patients and other sources, presented in 33(16%) patients.
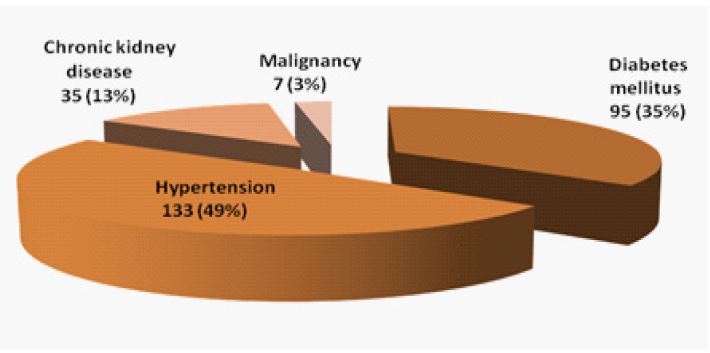
Chronic comorbid conditions
The pre-existing chronic co-morbidities Chronic kidney disease, Diabetes Mellitus, Malignancy and Hypertension were listed among severe sepsis, sepsis and septic shock patients. Hypertension presented in 133 patients (49%), Diabetes Mellitus presented in 95 patients (35%), Chronic kidney disease presented in 35 patients (13%) and Malignancy presented in 7 patients (3%).
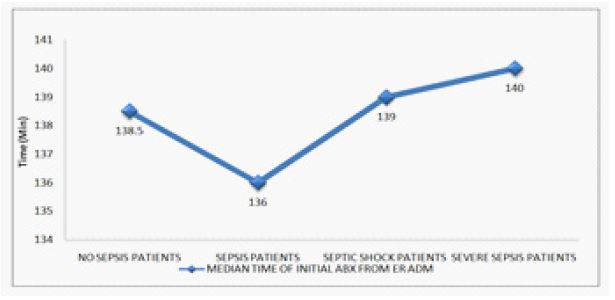
Initial antibiotic administration time (min) after emergency room admission
The median time between being admitted to the emergency room and receiving an antibiotic was 138.5 minutes for No sepsis patients (n=76), 136 minutes for Sepsis patients (n=127), 139 minutes for Severe sepsis patients (n=36) and 140 minutes for septic shock patients (n=45).
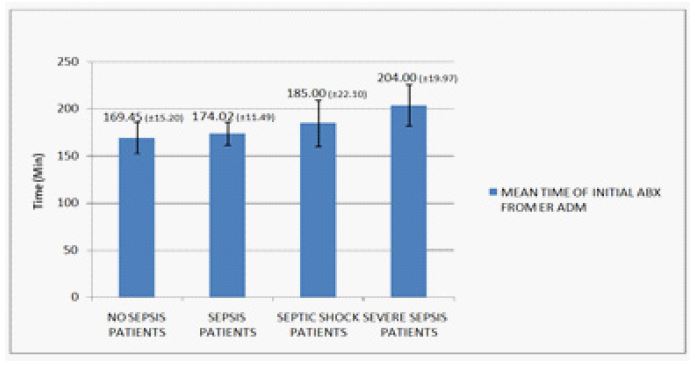
The mean time between being admitted to the emergency room and receiving an antibiotic was 169.45 for No sepsis patients (n=76), 174.02 minutes for Sepsis patients (n=127), 185 minutes for Severe sepsis patients (n=36) and 204 minutes for septic shock patients (n=45).
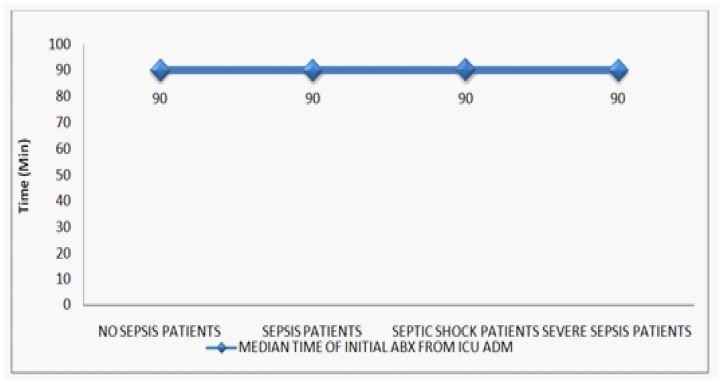
Initial antibiotic administration time (min) after being admitted to the Intensive Care Unit
The median time from being admitted to the Intensive Care Unit to initial antibiotic administration was 90 minutes for No sepsis patients (n=76), 90 minutes for Sepsis patients (n=127), 90 minutes for Severe sepsis patients (n=45) and 90 minutes for septic shock patients (n=36).
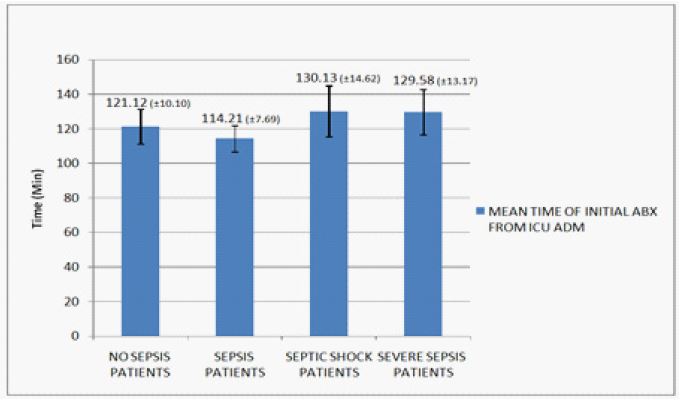
The mean time of initial antibiotic administration time (min) after ICU admission was 121.12 for No sepsis patients (n=76), 114.21 minutes for Sepsis patients (n=127), 130.13 minutes for Severe sepsis patients (n=36) and 129.58 minutes for septic shock patients (n=45).
Patient outcome in sepsis pateint population
Among 127 sepsis patients, only 45 received antibiotics within 1 hour of Intensive Care Unit admission, 79 received antibiotics within 1-6 hours of Intensive Care Unit admission, and 3 received antibiotics after 6 hours of Intensive Care Unit admission. Overall mortality in sepsis patients was 17/127 (13.39%).
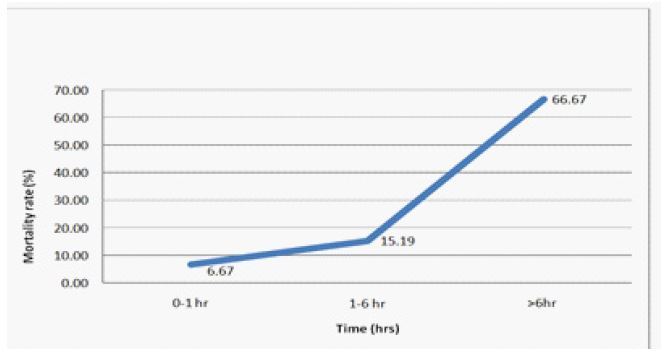
Figure 10 depicts the time from after being admitted to the Intensive Care Unit to initial antibiotics, sorted by the hospital’s ultimate result (percentage mortality). We discovered a correlation between in-hospital mortality and the time from after being admitted to the Intensive Care Unit to administration of antibiotics during the first 6 hours of resuscitation.
45(35.43%) patients, who were administered antibiotics within 60 min after Intensive Care Unit admission. When compared with patients who were received antibiotics after 1hr and within 6 hr (n=79) of Intensive Care Unit admission, patients receiving antibiotics after 1hr and within 6 hr had a elevation in the mortality percentage, 8.52% (OR=2.51), and patients receiving antibiotics after 6 hrs have a significantly elevation in mortality percentage, 51.48% (OR=11.17).
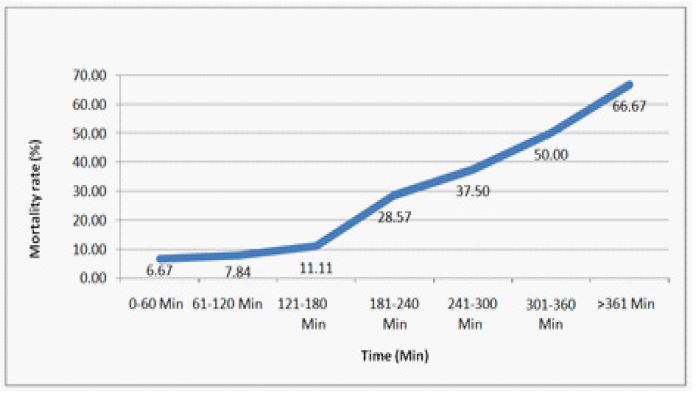
Figure 11 shows impact of initial antibiotic administration time (min) after Intensive Care Unit admission on the percentage mortality of sepsis Patients. We found elevation in mortality associated with delay to administration of antibiotics during the every hour after Intensive Care Unit admission. Mortality was 6.67% (lowest) if effective antimicrobials were administered within first hours of Intensive Care Unit admission, 7.84% in the second hour, 11.11% in the third hour, 28.57% in the fourth hour, 37.5% in the fifth hour, 50% in the sixth hour, and 66.67% (highest) in after sixth hour.
Patient outcome in severe sepsis patient population
Among 45 severe sepsis patients, only 16 received antibiotics within 1 hour of Intensive Care Unit admission, 28 received antibiotics within 1-6 hours of Intensive Care Unit admission, and 1 received antibiotics after 6 hours of Intensive Care Unit admission. Overall mortality in severe sepsis patients was 9/45 (20%).
Figure 12 depicts the time from Intensive Care Unit admission to initial antibiotics, stratified by final hospital outcome (Percentage mortality). We found association between in-hospital mortality and the time from Intensive Care Unit admission to administration of antibiotics during the first 6 hours of resuscitation. A total of 16 patients received antibiotics within 60 min after ICU admission. When compared with patients who received antibiotics after 1 hr and within 6 hr (n=28) of ICU admission, patients receiving antibiotics after 1 hr and within 6 hr had a raise in the mortality percentage, 18.75% (OR=5.00), and patients receiving antibiotics after 6 hrs have a significantly raise in mortality percentage, 75.00%.
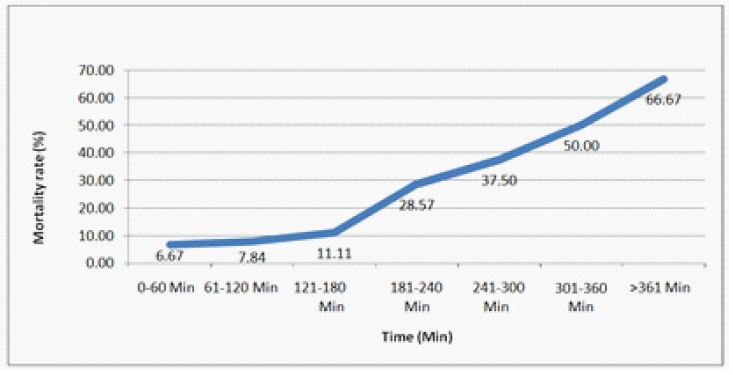
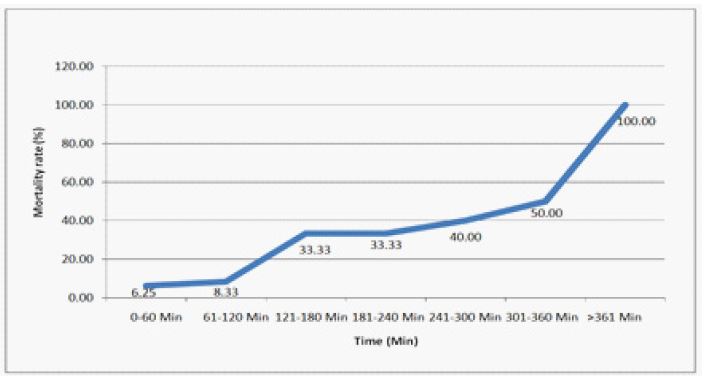
Figure 13 shows impact of initial antibiotic receiving time (min) after Intensive Care Unit admission on the percentage mortality of severe sepsis Patients. We discovered a correlation between an raise in fatality and prolonging administering of antibiotics during the every hour after Intensive Care Unit admission. Mortality was 6.25% (lowest) if effective antimicrobials were administered within first hours of Intensive Care Unit admission, 8.33% in the second hour, 33.33% in the third hour, 33.33% in the fourth hour (no change in mortality rate during fourth hour), 40.00% in the fifth hour, 50% in the sixth hour, and 100% (highest) in after sixth hour.
Patient outcome in septic shock pateint population
Among 36 septic shock patients, only ten patients were given antibiotics within 1 hour of Intensive Care Unit admission, 24 patients were given antibiotics within 1-6 hours of Intensive Care Unit admission and 2 patients were given antibiotics after 6 hours of Intensive Care Unit admission.
Overall mortality in septic shock patients was 52.78%. Altogether mortality rate is highest in Septic shock patients than severe sepsis and sepsis patients.
Figure 14 depicts the time from Intensive Care Unit admission to initial antibiotics, stratified by final hospital outcome (percentage mortality). We discovered a correlation between the length of time from ICU admission to the start of antibiotic administration during the first six hours of resuscitation and in-hospital mortality. Within 60 minutes of their Intensive Care Unit admission, total ten patients in all received antibiotics. Patients who received antibiotics after one hour and within six hours (n=24) of admission to the Intensive Care Unit had a high mortality rate (28.33%; OR=3.27), and those who received antibiotics after six hours had a significantly higher mortality rate (41.67%).
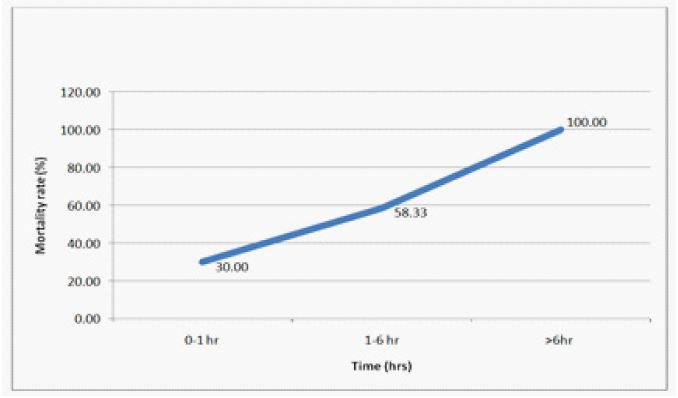
Figure 15 shows impact of initial treatment with antibiotics (minutes) after Intensive Care Unit admission on the percentage mortality of septic shock patients. We discovered a higher death rate when antibiotics failed to be given promptly during the first hour following Intensive Care Unit admission and every hour after that. Mortality was 30% (lowest) if effective antimicrobials were administered within first hours of ICU admission, 35.71% in the second hour, 40% in the third hour, 0% (no septic shock patient were given antibiotics in this hour during study period) in the fourth hour, 100% in the fifth hour, 100% in the sixth hour, and 100% in after sixth hour.
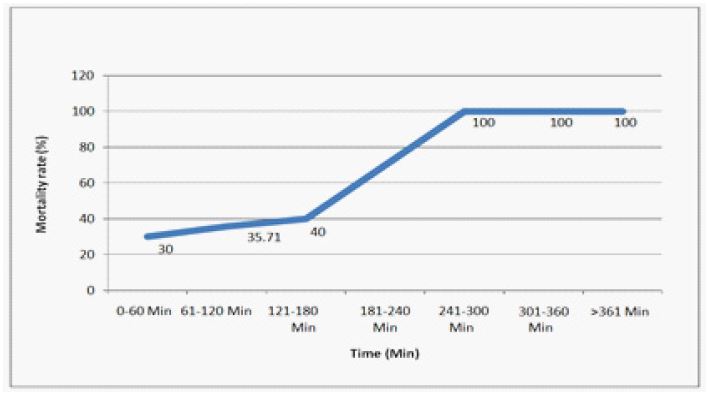
§The data point at 181-240 min time range is excluded from line graph since no subject is recorded within this range.
Microbiologic pathogens in severe sepsis, sepsis and septic shock
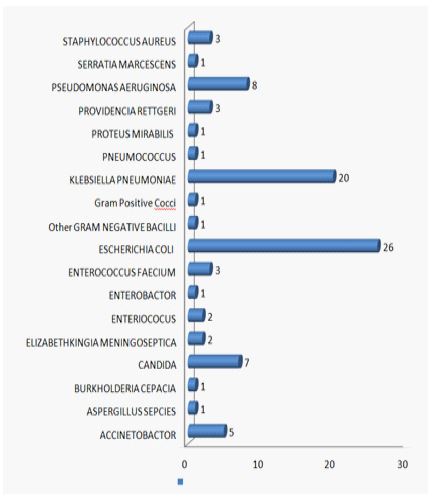
Of the 208 patients with severe sepsis, sepsis, and septic shock, 78(37.50%) had positive blood cultures for pathogenic organisms. Table 11 lists the organisms that were isolated from the samples (sputum, ETT, blood, urine, pus, and body fluid) along with the frequency at which they appeared in patients with severe sepsis, sepsis and septic shock.
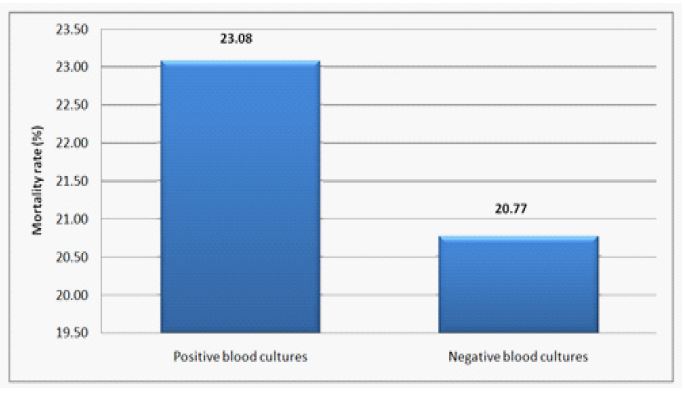
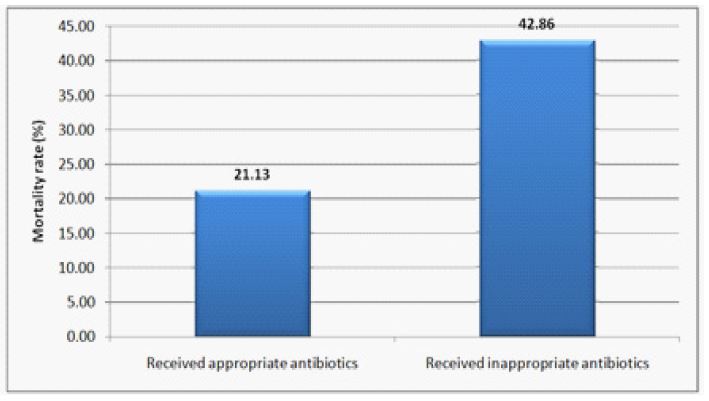
In contrast to 27/130 (20.77%) for blood culture negative infections (OR=1.14), the death rate for blood culture positive infections was 18/78 (23.08%). Seven patients did not receive the proper antibiotics, out of the 78 patients with positive blood cultures, and 71 of them received antibiotics in the intensive care unit (ICU) that the causative organism was susceptible to. Patients treated appropriately for blood culture positive severe sepsis, sepsis and septic shock infection in the intensive care unit had a mortality rate of 15/71 (21.13%) compared to 3/7 (42.86%) for those treated inappropriately (OR=2.80).
Figure 16 shows mortality graph in Positive blood cultures and negative blood cultures in severe sepsis, sepsis and septic shock patient population.
Figure 17 shows mortality graph in patient population of severe sepsis, sepsis and septic shock, who received appropriate antibiotics and inappropriate antibiotics according to their blood culture reports.
Discussion
The 10 months study includes 284 patients being admitted for severe sepsis, sepsis and septic shock or not affected by sepsis. The patient population exhibits a well-balanced age and sex distribution, with sepsis patients primarily classified into three severity categories: severe sepsis, sepsis and septic shock.
Infections that result into different types of sepsis include mostly renal (36%) and chest (21%) in this sample patient population. In these three types of sepsis highest co-morbidities are hypertension with 49% at first place followed by diabetes mellitus with 35%.
The lowest death rates were linked to starting an effective antimicrobial therapy within the first hour of being admitted to the Intensive Care Unit (ICU): 6.25% for patients with severe sepsis, 6.67% for patients with sepsis and 30% for patients in septic shock. In the initial six hours following ICU admission, the mortality rate rose by an average of 9.59% for patients with severe sepsis, 4.67% for patients with sepsis and 8.39% for patients experiencing septic shock for each extra hour until effective antimicrobial initiation was implemented.
The mortality rate for sepsis patients increased to 1.18% when effective antimicrobial therapy was started between the first and second hours after intensive care unit admission, and it was 50% when effective antimicrobial therapy was delayed until five or six hours after Intensive Care Unit admission. When effective antimicrobial therapy was started within the between the first and second hour of Intensive Care Unit admission, the mortality rate rose to 2.08%; however, when effective antimicrobial therapy was delayed until five or six hours after Intensive Care Unit admission, the mortality rate for patients with severe sepsis was 50%.
When effective antimicrobial therapy was started between the first and second hour of an Intensive Care Unit admission, the mortality rate rose to 5.71%; however, when effective antimicrobial therapy was delayed to 5-6 hrs after Intensive Care Unit admission, the mortality rate for patients suffering from septic shock was 100%. By the second hour following admission to the Intensive Care Unit, the odds ratio of death had increased significantly, and the ratio increased with longer delays. These results imply that a crucial therapeutic variable linked to the mortality from severe sepsis, sepsis and septic shock is the delay in starting an effective antimicrobial therapy after the Intensive Care Unit admission time.
For patients with sepsis, the median time from emergency admission to the administration of effective antimicrobial therapy was 136 minutes, and from ICU admission to that time it was 90 minutes. For patients with severe sepsis, the median time from emergency admission to the administration of effective antimicrobial therapy was 139 minutes, and from ICU admission to that time it was 90 minutes. For patients in septic shock, the median time from emergency admission to the administration of effective antimicrobial therapy was 140 minutes, whereas it was 90 minutes for ICU patients.
Within an hour of being admitted to the intensive care unit, 35.43% of all patients with sepsis received effective antimicrobial therapy. By three hours after ICU admission, 82.68% and 97.64% of patients by 6 hours had gotten them, respectively. Effective antimicrobial therapy was administered to 35.56% of all severe sepsis patients within the first hour of ICU admission, 75.56% by the third hour, and 97.78% by the sixth hour. Effective antimicrobial therapy was administered to 27.78% of all septic shock patients within the first hour of ICU admission, 80.56% by the third hour, and 88.89% by the sixth hour.
These results are anticipated. Within the first hour of diagnosing severe sepsis and septic shock, broad spectrum antibiotics should always be given, according to the international consensus guidelines of the Surviving Sepsis Campaign (SSC) [8]. A sizable retrospective study that was released in 2006 serves as the main foundation for this recommendation [9]. According to Kumar et al.’s study, patients who received antibiotics within the first hour of recorded hypotension went on to survival rate of 79.9%. For every hour that passed during the next six hours without antimicrobial therapy, the average reduction in survival was 7.6%. The data we provided in this report validated these conclusions.
Furthermore, a sufficient number of cases enable the proof that this mortality effect extends to patient subgroups in relation to pathogenic bacteria isolation and appropriate versus inappropriate antibiotic administration. This suggests that the underlying processes of infection are similar in all of these groups and highlights the significance of starting appropriately chosen therapy early on. Delays in initiating effective antimicrobial therapy harm survival rates for both patient groups with positive and negative cultures.
A healthcare professional can’t determine whether an antibiotic prescription is appropriate because the basis for antibiotic appropriateness is culture data, which is not available for 24 to 96 hours or further after the initial antibiotic administration. Therefore, using these criteria to assess how the timing of antibiotics affects results doesn’t seem right.
It’s interesting to note that this problem goes beyond semantics, especially in light of the high rate of culture-negative infections (62.50% in this study), which gives rise to two different standards of appropriateness depending on whether a positive culture is present or not. In addition, every study on infections needs to analyze the causative organism subjectively. Making such a determination is especially challenging when multiple cultures yield positive results for different organisms. The data on antibiotic sensitivity and pathogenic organisms have made appropriateness of antibiotics a significant confounding factor in our results [10].
There are a few issues with this study that should be taken into account. First, only 24-hour time intervals were reported, and the study’s overall mortality rate of 21.63% was meager. Second, nearly all of patients received antibiotics within three hours of being evaluated, and as time points get longer, it becomes more challenging to draw firm conclusions about associations due to the relatively small numbers of patients in the subsequent time points and the wide confidence intervals. Evidently, more information is required to understand the connection between patient outcome and time to source control.
In general, compliance with sepsis guideline recommendations was poor. Only one-third patients received their first antimicrobial agent according to current guideline recommendations before or within 1 hour of ICU admission of severe sepsis, sepsis and septic shock patient population.
Within this patient population it was noted that patients are mostly affected with Escherichia coli and Klebsiella pneumoniae with 30% and 23% respectively. Mortality rate is greater in the patients with positive blood cultures than with negative blood cultures by an odds ratio of 1.14 (>1), and an even more intriguing discovery is that, with an odds ratio of 2.80 (>1), the mortality rate for patients who did not receive the proper antibiotic treatment is higher than that of patients who received it. This means that patients with positive blood cultures who are not given the right antibiotics have a higher chance of dying. Other studies have also shown an increase in mortality in patients with inappropriate initial antibiotic treatment [11,12].
The study included the prospective data collection and single center design. Patient population has a good demography of age and sex distribution. This study used short-term prospective data collection and is therefore not influenced by secular trends. This study is well organized by categorization of the patient population into different categories of sepsis severity and data points are finely differentiated with antibiotic administration time. This study also includes the microbiological assessment of patient groups that reveals the evidence of pathogens responsible for mortality and effectiveness of appropriate antibiotic administration.
Conclusion
We were able to show a correlation between hospital mortality and the timing of antibiotic administration following Intensive Care Unit admission in this prospective study of patients with severe sepsis, sepsis, and septic shock who received effective antimicrobial therapy after Intensive Care Unit admission. Increased mortality was linked to even a one-hour delay in the administration of antibiotics following their admission in the intensive care unit.
The lowest death rates were linked to starting effective antimicrobial therapy within the first hour of being admitted to the intensive care unit. These rates were 6.67% (lowest) for patients with sepsis (Figure 10), 6.25% (lowest) for patients with severe sepsis (Figure 12), and 30% (lowest) for patients with septic shock (Figure 14). In the first six hours following admission to the Intensive Care Unit, the mortality rate rose by an average of 4.67% for patients with sepsis, 9.59% for patients with severe sepsis, and 8.39% for patients experiencing septic shock for each extra hour that effective antimicrobial initiation was delayed. All patients with severe sepsis, sepsis, and septic shock had an increasing mortality rate with an increasing duration of initial antibiotic administration.
More data on the relationship between time to source control and patient result are needed. Adequacy of empirical antibiotic treatment is important for the survival in severe sepsis, sepsis and septic shock and choice of initial antibiotic treatment is an important decision in the therapy of these patients. The effect of the timing of antibiotic treatment on sepsis, severe sepsis, and septic shock mortality was only indirectly supported by the available data, and there is considerable variation in the evidence regarding this matter. Therefore, randomized controlled trials are required to clarify the effects of timing antibiotic treatment on survival. Initiatives for improving quality of care should not be limited to sepsis; instead, they should concentrate on the prompt identification and appropriate management of infections in order to stop them from developing into severe sepsis and septic shock.
It is quite evident in this research study and other similar studies that, how critical the time factor is for survival of sepsis patients. In summary, severe sepsis, sepsis and septic shock are time critical diseases, and therefore, one of significant concern to the medicine physician. To the cardiologist, “time is muscle,” to the neurologist, “time is brain”, to the physician caring for the septic patient, “time is survival.”
References
- Roach AC. Antibiotic therapy in septic shock. Crit Care Nurs Clin North Am. 1990; 2(2): 179-86. PMID: 2192726.
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001; 29(7): 1303-10. doi: 10.1097/00003246-200107000-00002. PMID: 11445675.
- Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM, Jaeschke R, Reinhart K, Angus DC, Brun-Buisson C, Beale R, Calandra T, Dhainaut JF, Gerlach H, Harvey M, Marini JJ, Marshall J, Ranieri M, Ramsay G, Sevransky J, Thompson BT, Townsend S, Vender JS, Zimmerman JL, Vincent JL; International Surviving Sepsis Campaign Guidelines Committee; American Association of Critical-Care Nurses; American College of Chest Physicians; American College of Emergency Physicians; Canadian Critical Care Society; European Society of Clinical Microbiology and Infectious Diseases; European Society of Intensive Care Medicine; European Respiratory Society; International Sepsis Forum; Japanese Association for Acute Medicine; Japanese Society of Intensive Care Medicine; Society of Critical Care Medicine; Society of Hospital Medicine; Surgical Infection Society; World Federation of Societies of Intensive and Critical Care Medicine. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med. 2008; 36(1): 296-327. doi: 10.1097/01.CCM.0000298158.12101.41. Erratum in: Crit Care Med. 2008; 36(4): 1394-6. PMID: 18158437.
- Leibovici L, Paul M, Poznanski O, Drucker M, Samra Z, Konigsberger H, Pitlik SD. Monotherapy versus beta-lactam-aminoglycoside combination treatment for gram-negative bacteremia: a prospective, observational study. Antimicrob Agents Chemother. 1997; 41(5): 1127-33. doi: 10.1128/AAC.41.5.1127. Erratum in: Antimicrob Agents Chemother 1997 Nov;41(11):2595. PMID: 9145881; PMCID: PMC163862.
- Ibrahim EH, Sherman G, Ward S, Fraser VJ, Kollef MH. The influence of inadequate antimicrobial treatment of bloodstream infections on patient outcomes in the ICU setting. Chest. 2000; 118(1): 146-55. doi: 10.1378/chest.118.1.146. PMID: 10893372.
- Dellinger RP, Carlet JM, Masur H, Gerlach H, Calandra T, Cohen J, Gea-Banacloche J, Keh D, Marshall JC, Parker MM, Ramsay G, Zimmerman JL, Vincent JL, Levy MM; Surviving Sepsis Campaign Management Guidelines Committee. Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Crit Care Med. 2004 Mar;32(3):858-73. doi: 10.1097/01.ccm.0000117317.18092.e4. Erratum in: Crit Care Med. 2004 Jun;32(6):1448. Dosage error in article text. Erratum in: Crit Care Med. 2004; 32(10): 2169-70. PMID: 15090974.
- Bayarski Y. Antibiotics and Their Types, Uses and Side Effects. Dari: http://hamiltoncountypreppers. org/. Diakses. 2006;12.
- Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, Sevransky JE, Sprung CL, Douglas IS, Jaeschke R, Osborn TM, Nunnally ME, Townsend SR, Reinhart K, Kleinpell RM, Angus DC, Deutschman CS, Machado FR, Rubenfeld GD, Webb SA, Beale RJ, Vincent JL, Moreno R; Surviving Sepsis Campaign Guidelines Committee including the Pediatric Subgroup. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013; 41(2): 580-637. doi: 10.1097/CCM.0b013e31827e83af. PMID: 23353941.
- Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, Peterson E, Tomlanovich M; Early Goal-Directed Therapy Collaborative Group. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001; 345(19): 1368-77. doi: 10.1056/NEJMoa010307. PMID: 11794169.
- Puskarich MA, Trzeciak S, Shapiro NI, Arnold RC, Horton JM, Studnek JR, Kline JA, Jones AE; Emergency Medicine Shock Research Network (EMSHOCKNET). Association between timing of antibiotic administration and mortality from septic shock in patients treated with a quantitative resuscitation protocol. Crit Care Med. 2011; 39(9): 2066-71. doi: 10.1097/CCM.0b013e31821e87ab. PMID: 21572327; PMCID: PMC3158284.
- Harbarth S, Garbino J, Pugin J, Romand JA, Lew D, Pittet D. Inappropriate initial antimicrobial therapy and its effect on survival in a clinical trial of immunomodulating therapy for severe sepsis. Am J Med. 2003; 115(7): 529-35. doi: 10.1016/j.amjmed.2003.07.005. PMID: 14599631.
- Lodise TP, McKinnon PS, Swiderski L, Rybak MJ. Outcomes analysis of delayed antibiotic treatment for hospital-acquired Staphylococcus aureus bacteremia. Clin Infect Dis. 2003; 36(11): 1418-23. doi: 10.1086/375057. Epub 2003 May 20. PMID: 12766837.