
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Venous thrombosis revealing Crohn’s disease in pediatrics: A case report
S Hani*; R Dahni; R El Qadiry; H Nassih; A Bourrahouat; I Ait Sab
Department of Pediatrics B, Mother and Child Hospital, Mohamed VI Marrakech University Hospital Center, Morocco.
*Corresponding Author : S Hani
Department of Pediatrics B, Mother and Child Hospital, Mohamed VI Marrakech University Hospital Center, Morocco.
Email: dr.sorayahani@gmail.com
Received : Dec 01, 2023
Accepted : Dec 28, 2023
Published : Jan 04, 2024
Archived : www.jcimcr.org
Copyright : © Hani S (2024).
Abstract
Thromboembolic events are severe but classic complications of chronic Inflammatory Bowel Disease (IBD). They are attributed to a pre-thrombotic state induced by the inflammatory activity of this disease. Most often, these are venous thrombosis of the limbs and pulmonary embolism. Cerebral venous thrombosis is rarely described during the course of CD, and remains exceptional as an inaugural manifestation. We report an observation of Crohn’s disease revealed by bilateral thrombophlebitis of the lower limbs.
After confirmation by imaging, the patient’s aetiological investigation revealed digestive disorders that had been evolving for 6 months, with a severe delay in weight and height, prompting a colonoscopy confirming the diagnosis of crohn’s disease. The patient was put on an antivitamin K anticoagulant, with induction treatment based on partial enteral nutrition (Modulen IBD) combined with corticosteroid therapy and bi-antibiotic therapy based on metronidazole and ciprofloxacin. The evolution was favourable, marked by a clinical-radiological improvement, as well as a biological improvement, notably the normalization of the haemostasis balance.
Despite the high risk of thromboembolic events in IBD, data are limited and there are no anticoagulation guidelines for paediatric patients. It is therefore important to study pathophysiological mechanisms, identify incriminating risk factors, and the particularities of management and prevention for these patients.
Keywords: Thrombophlebitis; Crohn’s disease; Prevention; Chronic Inflammatory Bowel Disease (IBD).
Citation: Hani S, Dahni R, El Qadiry R, Nassih H, Bourrahouat A, et al. Venous thrombosis revealing Crohn’s disease in pediatrics: A case report. J Clin Images Med Case Rep. 2024; 5(1): 2777.
Introduction
Thromboembolic events are an extra-intestinal manifestation of crohn’s disease that can cause considerable morbidity and mortality.
Studies suggest that patients suffering from Inflammatory Bowel Disease (IBD) may be 2 to 3 times more at risk than those who do not, with a predilection for occurrence during the active phase of the disease.
We report the case of a 13-year-old child diagnosed with crohn’s disease revealed by bilateral thrombophlebitis of the lower limbs in the pediatric ward B during the year 2023 at the CHU Mohammed VI in Marrakech.
Objective: In this case, we report the clinical, paraclinical and evolutionary profile of a patient diagnosed with crohn’s disease revealed by bilateral thrombophlebitis of the lower limbs, a potentially serious and frequent complication during IBD.
Clinical observation
14-year-old child initially admitted for left calf pain evolving for 1 month with sensation of heaviness in the leg, with a history of glairo-bloody diarrhea evolving for 6 months in relapses and remissions with no other associated signs, all evolving in a context of altered general condition and weight loss not quantified.
Clinical examination revealed a pale, hemodynamically and respiratorily stable patient, malnourished, with -3DS staturo-ponderal retardation, and on examination of the lower limbs, a palpable, warm, painful subcutaneous linear cord opposite the course of the left saphenous vein, with a positive Homans’ sign. Examination of the anal margin revealed two vertical anterior and posterior anal fissures, with circumferential external hemorrhoids and a clean finger pad on rectal examination.
Biological workup revealed microcytic hypochromic anemia of inflammatory origin, prothrombin level 62%, low INR 1.02, elevated fecal calprotectin 580 ug/g, positive Anti-Saccharomyces Cerevisiae Ac (ASCA).
Doppler ultrasound revealed thrombophlebitis of both lower limbs, extending to the subrenal inferior vena cava.
Abdominal ultrasound revealed circumferential and pancolic parietal thickening and thickening of the last ileal loop, associated with extensive diffuse infiltration of mesenteric fat of probable inflammatory origin.

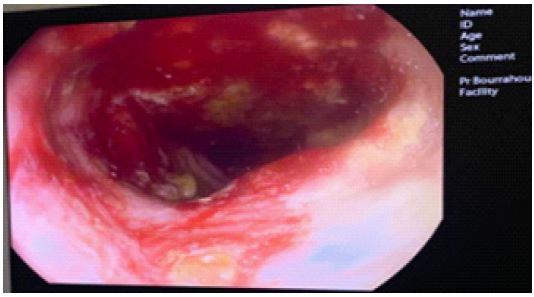
Colonoscopy revealed multiple deep ulcerations with pseudopolyps extending from the rectum to the left colonic angle, with swollen, inflamed mucosa bleeding easily.
Pathological examination of colonic and ileal biopsies revealed transmural inflammation with epithelioid histiocytes without crypt involvement, in favor of crohn’s disease.
The patient was initially put on induction therapy with partial enteral nutrition.
(Modulen IBD) combined with corticosteroid therapy and bi-antibiotic therapy based on metronidazole and ciprofloxacin, with anticoagulant treatment based on antivitamin K.
Given our patient’s high level of inflammatory activity, treatment with biotherapy was envisaged, but due to lack of resources, treatment with an immunosuppressant based on Azathioprine was chosen.
The patient’s outcome was favorable, with clinical improvement in the form of regression of pain in the lower limbs, weight regain, normalization of transit and healing of anal fissures, as well as biological improvement, notably normalization of hemostasis.
Discussion
In addition to digestive lesions, IBD can induce numerous extra-intestinal manifestations, including thromboembolic complications. Thromboembolic disease is more common in active or complicated IBD [1]. However, 30 to 40% of thromboses occur in the quiescent phase [2-5].
Vascular Thrombosis (VT) is more often venous than arterial, dominated by thrombosis of the deep veins of the lower limbs, portal veins and cerebral veins [2,6]. Their pathogenesis is probably multifactorial, resulting from interactions between hereditary and acquired risk factors.
The clinical characteristics of children with IBD and associated thromboembolic events have been evaluated by retrospective studies [7], which highlighted acquired risk factors including ileocolonic involvement and disease complicated by fistulae, strictures, abscesses and recent surgery in patients with crohn’s disease.
Acquired risk factors for thrombosis in IBD include, in addition to those known in the general population, factors related to the disease itself [8], such as inflammation [9,10], impaired coagulation and fibrinolysis [11,12], platelet abnormalities [13,14], anemia [15], hyperhomocysteinemia [16,17], antiphospholipid antibody positivity [18], malabsorption, surgery and drugs [19]. Inherited risk factors include mutations involving FVL, factor II (prothrombin G20210A), MTHFR 6777T [20] and the PAI-1 gene polymorphism [21], which, although rare in IBD patients, increase the risk of thrombosis when present.
Diamond et al [22] showed a high rate of Central Venous Catheter (CVC)-related thrombosis in pediatric IBD patients, and also demonstrated a decrease in the incidence of CVC-related thrombosis with the use of prophylactic anticoagulation. In addition, use of a large inpatient database revealed an increased risk of thrombosis and infection in IBD patients receiving parenteral nutrition via CVC [23]. Steroid use has also been identified as a risk factor for Venous Thromboembolism (VTE). Experimental studies have shown that steroid treatment increases coagulation factor and fibrinogen levels [24,25]. In a meta-analysis assessing the risk of VTE in IBD patients with or without systemic corticosteroid treatment, a significantly higher rate of VTE complications was noted in steroid-treated IBD patients than in non-steroid-exposed patients.
The pathogenesis of these thromboembolic events has been associated with increased activation of the coagulation cascade, impaired fibrinolysis, increased platelet counts and endothelial dysfunction [26,27].
Inherited prothrombotic disorders are no more prevalent in the IBD population than in the general population [26,28]. Interestingly, the majority of patients tested for FVIII had elevated levels. FVIII is an acute-phase reagent often elevated in inflammatory states and has been shown to be an independent risk factor for TVE.
Unfortunately, while there are guidelines for prophylaxis and treatment in adults, there are none for pediatric IBD patients [29], but only for children with UC, requiring surgery or in patients at high risk of thromboembolic events [30,31]. In these cases, prophylaxis is recommended.
In addition, the latest ECCO/ESPGHAN guideline updates since the recent pandemic recommend prophylaxis in all hospitalized IBD patients with severe acute colitis, regardless of age, due to the additional pro-thrombotic risk associated with coronavirus 2019 disease [32].
In fact, it is suggested that the role of factors involved in a hypothetical thromboembolic event in children, as well as prevention strategies, still need to be well defined, including an accurate family history of thromboembolic events, careful laboratory evaluation of acquired and congenital risk factors, should already be performed when evaluating pediatric IBD patients.
Finally, multicenter studies on a larger patient population are needed to accurately characterize the role of thromboembolic risk factors in children with IBD, and to plan prevention strategies from pediatric age onwards, in order to highlight likely long-term lesions and the long-term effects of preventive therapy.
Conclusion
Pediatric IBD patients are at risk of thromboembolism, although the absolute risk remains relatively low. The safety and efficacy of pharmacological thromboprophylaxis need to be further evaluated in this population, taking into account the incriminating risk factors.
References
- Twig G, Zandman-Goddard G, Szyper-Kravitz M, et al. Systemic thromboembolism in inflammatory bowel disease: Mechanisms and clinical applications. Ann N Y Acad Sci. 2005; 1051: 166-73.
- Talbot RW, Heppell J, Dozois RR, et al. Vascular complications of inflammatory bowel disease. Mayo Clin Proc. 1986; 61: 140-145
- Owczarek D, Cibor D, Głowacki MK, Rodacki T, Mach T. Inflammatory bowel disease: Epidemiology, pathology and risk factors for hypercoagulability. World J Gastroenterol. 2014; 20: 53-63.
- Milandre L, Monges D, Dor V, et al. Cerebral phlebitis and Crohn disease. Rev Neurol. 1992; 148: 139-44.
- Miehsler W, Reinisch W, Valic E, et al. Is inflammatory bowel disease an independent and disease specific risk factor for thromboembolism? Gut. 2004; 53: 542-8.
- Webberley MJ, Hart MT, Melikian V. Thromboembolism in inflammatory bowel disease: Role of platelets. Gut. 1993; 34: 24751.
- Coremans L, Strubbe B, Peeters H. Venous thromboembolism in patients with inflammatory bowel disease: review of literature and practical algorithms. Acta Gastroenterol Belg. 2021; 84: 79-85.
- Danese S, Papa A, Saibeni S, et al. Inflammation and coagulation in inflammatory bowel disease: The clot thickens. Am J Gastroenterol. 2007; 102: 174-186.
- Grainge MJ, West J, Card TR. Venous thromboembolism during active diseases and remission in inflammatory bowel diseases: a cohort study. Lancet. 2010; 375: 657-663.
- Yazicia A, Senturk O, Aygun C, et al. Thrombophilic risk factors in patients with inflammatory bowel disease. Gastroenterol Res. 2010; 3: 112-119.
- Kume K, Yamasaki M, Tashiro M, et al. Activations of coagulation and fibrinolysis secondary to bowel inflammation in patients with ulcerative colitis. Intern Med. 2007; 46: 1323-1329.
- Chiarantini E, Valanzano R, Liotta AA, et al. Hemostatic abnormalities in inflammatory bowel disease. Thromb Res. 1996; 82: 137-146.
- Webberley MJ, Hart MT, Melikian V. Thromboembolism in inflammatory bowel disease: Role of platelets. Gut. 1993; 34: 247-251.
- Yoshida H, Granger DN. Inflammatory bowel disease: A paradigm for the link between coagulation and inflammation. Inflamm Bowel Dis. 2009; 15: 1245-1255.
- Katsanos AH, Kosmidou M, Giannopoulos S, et al. Cerebral arterial infarction in inflammatory bowel diseases. Eur J Intern Med. 2014; 25: 37-44.
- Oussalah A, Gueant JL, Peyrin-Biroulet L. Meta-analysis: Hyperhomo- cysteinaemia in inflammatory bowel diseases. Aliment Pharmacol Ther. 2011; 34: 1173-1184.
- Cattaneo M, Vecchi M, Zighetti ML, et al. High prevalence of hyper- homocysteinemia in patients with inflammatory bowel disease: A pathogenetic link with thromboembolic complications? Thromb Haemost. 1998; 80: 542-545.
- Koutroubakis IE, Petinaki E, Anagnostopoulou E, et al. Anticardiolipin and anti-beta2-glycoprotein I antibodies in patients with inflammatory bowel disease. Dig Dis Sci. 1998; 43: 2507-2512.
- Koutroubakis IE, Sfiridaki A, Tsiolakidou G, et al. Genetic risk factors in patients with inflammatory bowel disease and vascular complications: case-control study. Inflamm Bowel Dis. 2007; 13: 410-415.
- Mahmud N, Molloy A, McPartlin J, et al. Increased prevalence of methylenetetrahydrofolate reductase C677T variant in patients with inflammatory bowel disease, and its clinical implications. Gut. 1999; 45: 389-394.
- Levine A, Griffiths A, Markowitz J, et al. Pediatric modification of the Montreal classification for inflammatory bowel disease: The Paris classification. Inflamm Bowel Dis. 2011; 7: 1314-1321.
- Diamond CE, Hennessey C, Meldau J, et al. Catheter-related venous thrombosis in hospitalized pediatric patients with inflammatory bowel disease: Incidence, characteristics, and role of anticoagulant thromboprophylaxis with enoxaparin. J Pediatr 2018; 198: 53-59.
- Egberg MD, Galanko JA, Barnes EL, et al. Thrombotic and infectious risks of parenteral nutrition in hospitalized pediatric inflammatory bowel disease. Inflamm Bowel Dis. 2019; 25: 601-609.
- Sarlos P, Szemes K, Hegyi P, et al. Steroid but not biological therapy elevates the risk of venous thromboembolic events in inflammatory bowel disease: A meta-analysis. J Crohns Colitis. 2018; 12: 489-498
- van Zaane B, Nur E, Squizzato A, et al. Systematic review on the effect of glucocorticoid use on procoagulant, anti-coagulant and fibrinolytic factors. J Thromb Haemost. 2010; 8: 2483-2493.
- Danese S, Papa A, Saibeni S, et al. Inflammation and coagulation in inflammatory bowel disease: The clot thickens. Am J Gastroenterol. 2007; 102: 174-186.
- Giannotta M, Tapete G, Emmi G, et al. Thrombosis in inflammatory bowel diseases: what’s the link? Thromb J. 2015; 13: 14.
- Zhong M, Dong XW, Zheng Q, et al. Factor V Leiden and thrombosis in patients with inflammatory bowel disease (IBD): A meta-analysis. Thromb Res. 2011; 128: 403-409.
- Turner D, Ruemmele FM, Orlanski-Meyer E, et al. Management of paediatric ulcerative colitis, part 1: ambulatory care-an evidence-based guideline from European Crohn’s and Colitis Organization and European Society of Paediatric Gastroenterology, Hepatology and Nutrition. J Pediatr Gastroenterol Nutr. 2018; 67: 257-291.
- Hansen R, Meade S, Beattie RM, et al. Adaptations to the current ECCO/ESPGHAN guidelines on the management of paediatric acute severe colitis in the context of the COVID-19 pandemic: A RAND appropriateness panel. Gut 2021; 70: 1044-1052.
- Turner D, Ruemmele FM, Orlanski-Meyer E, et al. Management of paediatric ulcerative colitis, part 2: Acute severe colitis-an evidence-based consensus guideline from the European Crohn’s and Colitis Organization and the European Society of Paediatric Gastroenterology, Hepatology and Nutrition. J Pediatr Gastroenterol Nutr. 2018; 67: 292-310.
- Hansen R, Meade S, Beattie RM, et al. Adaptations to the current ECCO/ESPGHAN guidelines on the management of paediatric acute severe colitis in the context of the COVID-19 pandemic: A RAND appropriateness panel. Gut 2021; 70: 1044-1052.