
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Cerebral hydatid cyst masquerading as multiple cystic metastases: A rare presentation
Areeba Tariq*; Masqoob Talib; Manzar Hoseyn
Yong Loo Lin School of Medicine, National University of Singapore, Singapore.
*Corresponding Author : Areeba Tariq
Yong Loo Lin School of Medicine, National University of Singapore, Singapore.
Email: dr.areeba.tariq@gmail.com
Received : Dec 02, 2023
Accepted : Dec 28, 2023
Published : Jan 04, 2024
Archived : www.jcimcr.org
Copyright : © Tariq Aa (2024).
Citation: Tariq A, Talib M, Hoseyn M. Cerebral hydatid cyst masquerading as multiple cystic metastases: A rare presentation. J Clin Images Med Case Rep. 2024; 5(1): 2778.
Introduction
Hydatid disease, caused by encysted larvae of the dog tapeworm Echinococcus granulosus, results in the formation of proctoscoleces. The primary definitive host of the adult worm is the dog, while intermediate hosts for the larval stage include sheep and humans. Human infection occurs through the ingestion of food contaminated with ova or direct contact with infected dogs. Cerebral hydatidosis is a rare central nervous system larval infection affecting approximately 2-3% of patients, with the incidence of hydatid cysts among intracranial space-occupying lesions varying between 1.6 and 5.2 percent in different countries [1].
Case details
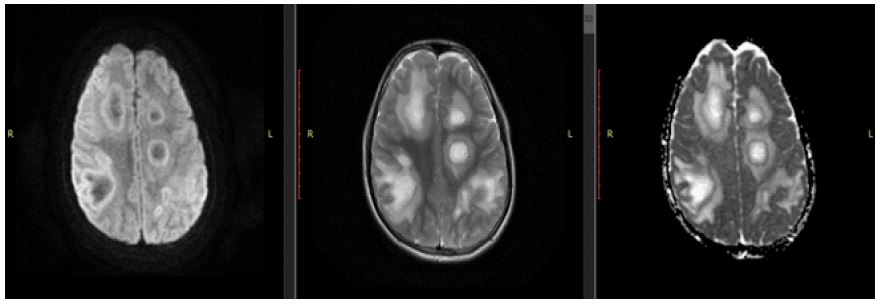
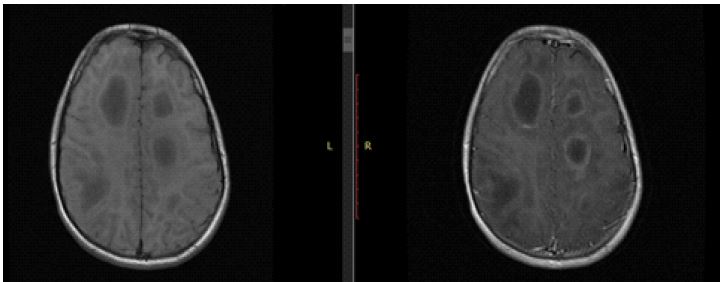
A 16-year-old boy, previously in good health, initially presented to the Emergency Department after a fall following vertigo. Being vitally and clinically stable, he was discharged, from the emergency room. Two days later, he returned with progressive weakness in the right upper and lower limbs. On arrival, his Glasgow Coma Scale (GCS) was 15, but he exhibited reduced strength in various muscle groups on the right side (right hemiparesis). CT and MRI scans of the brain with IV contrast revealed multiple well-defined cystic areas in the bilateral frontal and parietal regions, accompanied by moderate surrounding edema and peripheral ring enhancement on post-contrast images (Figures 1 and 2). The largest lesion, measuring 3.8x3.3x2.3 cm, was seen in the left frontal lobe. Abscess was ruled out due to the absence of restriction on the DWI sequence, leading to an initial impression of cystic metastasis. A subsequent CT of the chest, abdomen, and pelvis failed to identify a primary source, prompting a biopsy. Burr hole craniostomy with neuro navigation was planned. During surgery a grayish cyst-like structure was identified, which was biopsied. Postoperatively, the patient remained stable with mild right hemiparesis, and was discharged. During subsequent follow up in the clinic, his hemiparesis improved with no residual deficit. Histopathology indicated glial tissue with increased cellularity of lymphocytes and histiocytes (CD 68+). The presence of round to oval organisms within histiocytes led to the impression of an infected etiology, prompting referral to an infectious disease specialist. Positive echinococcus titre and other tests confirmed the diagnosis, and the patient commenced albendazole treatment, with ongoing clinic follow-ups.
Discussion
Hydatid disease, also known as echinococcosis, is a zoonotic parasitic infection transmitted from animals to humans through the larval stage of tapeworms (cestodes) belonging to the genus Echinococcus. In regions where echinococcosis is endemic, the World Health Organization (WHO) estimates an annual incidence of human infection exceeding 50/100,000 persons [2]. Approximately 1-2% of cases involve hydatid cysts affecting the human brain. Children constitute 80% of cases with brain involvement, often associated with dysfunctional valves or patent ductus arteriosus, primarily affecting the middle cerebral artery region [3]. The clinical manifestation of brain hydatid cysts is determined by their size and location, commonly presenting with symptoms such as hemiparesis, convulsions, migraines, vomiting, altered behavior, and even skull deformities. Over half of patients exhibit multiple cysts, predominantly in the cerebral hemispheres but also reported in various other brain regions [4].
Brain hydatid cysts appear as well-circumscribed cystic lesions on CT and MRI scans, rarely displaying daughter cysts. They typically lack wall calcification or surrounding edema, presenting only Cerebrospinal Fluid (CSF) density on CT or signal intensity on MRIs. Hypo intense rims on T2-weighted images are characteristic, with a low signal intensity rim surrounding the cyst visible on T2-weighted MRIs [5]. Cysts may appear non-complex or complicated, the latter involving per cystic edema due to rupture and leakage [6]. Non-complicated cysts on MRI are well-defined and isointense, lacking rim enhancement or pericystic edema. Conversely, complex cysts with superadded infections exhibit hyper intense pericystic edema and a ring of enhancement, either fully or partially, due to cyst rupture, making them prone to recurrence. Brain hydatid cysts should be considered in the differential diagnosis of cystic lesions, along alongside conditions like arachnoid cysts, porencephalic cysts, pyogenic abscesses, neurocysticercosis, and brain metastasis [7].
A high degree of suspicion is crucial when encountering cerebral cystic lesions on imaging, especially in regions with a high prevalence of hydatid disease, to ensure early diagnosis [8]. Despite limited studies in the region, Nasir et al. reported 33 cases of cerebral hydatid cysts, all appearing as isolated cystic masses on imaging. Clinicians suspected over 67% of these lesions to be hydatid cysts, with histopathological examination revealing transparent, thin-walled, unilocular, or multilocular cysts in 52% of cases. The intact cysts had an average size of 7 cm, displaying standard histology and responding well to medical treatment following surgical excision [9]. Total surgical extirpation is the therapeutic approach, emphasizing the importance of early diagnosis for favorable prognosis. Recurrence and unfavorable outcomes are commonly associated with incomplete excision and surgical rupture, necessitating careful removal to prevent anaphylaxis and widespread infection [10]. Dowling’s technique is the preferred surgical approach [11], and postoperatively, patients are administered antiparasitic drugs such as Albendazole or Mebendazole for 6-12 months in most cases, with doses ranging from 10-15 mg/kg in divided doses [12]. The results of pharmacological treatment vary across series, with response rates ranging from 43.5 to 80%. Early diagnosis significantly contributes to a favorable prognosis by preventing neurological consequences.
References
- Alshoabi SA, Alkalady AH, Almas KM, Magram AO, Algaberi AK, et al. Hydatid Disease: A Radiological Pictorial Review of a Great Neoplasms Mimicker. Diagnostics. 2023; 13: 1127.
- Torgerson PR, Devleesschauwer B, Praet N, Speybroeck N, Willingham AL, et al. World Health Organization Estimates of the Global and Regional Disease Burden of 11 Foodborne Parasitic Diseases, 2010: A Data Synthesis. PLoS medicine. 2015; 12: e1001920.
- Arega G, Merga G, Tafa G, Salah FO, Abebe G, et al. Temporoparietal Brain Hydatid Cyst in an Eight-Year-Old Child: A Rare Case Report. Pediatric health, medicine and therapeutics. 2022; 13: 361-5.
- Duransoy YK, Mete M, Barutçuoğlu M, Unsal U, Selçuki M. Intracranial hydatid cyst is a rare cause of midbrain herniation: A case report and literature review. Journal of pediatric neurosciences. 2013; 8: 224-7.
- Abbasi B, Akhavan R, Ghamari Khameneh A, Darban Hosseini Amirkhiz G, Rezaei-Dalouei H, et al. Computed tomography and magnetic resonance imaging of hydatid disease: A pictorial review of uncommon imaging presentations. Heliyon. 2021; 7: e07086.
- Abbassioun K, Rahmat H, Ameli NO, Tafazoli M. Computerized tomography in hydatid cyst of the brain. Journal of neurosurgery. 1978; 49: 408-11.
- Turgut M. Intracranial hydatidosis in Turkey: Its clinical presentation, diagnostic studies, surgical management, and outcome. A review of 276 cases. Neurosurgical review. 2001; 24: 200-8.
- Padayachy LC, Dattatraya M. Hydatid disease (Echinococcus) of the central nervous system. Child’s nervous system : ChNS: Official journal of the International Society for Pediatric Neurosurgery. 2018; 34: 1967-71.
- Din NU, Raza M, Rahim S, Memon W, Ahmad Z. Hydatid disease of central nervous system, a clinicopathological study of 33 cases. Journal of neurosciences in rural practice. 2023; 14: 293-7.
- Gezen F, Baysefer A, Köksel T, Gönül E, Akay KM, et al. Hydatid cysts of the brain. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 1995; 21: 938-42.
- Hage P, Salle H, Ibrahim I, Khalil W. Hydatid cyst excision using Dowling’s technique of hydrodissection. Acta neurochirurgica. 2022; 164: 2851-4.
- Dehkordi AB, Sanei B, Yousefi M, Sharafi SM, Safarnezhad F, et al. Albendazole and Treatment of Hydatid Cyst: Review of the Literature. Infectious disorders drug targets. 2019; 19: 101-4.