
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Non-recurrent laryngeal nerve: An anatomical variation in thyroid surgery
Chandrani Chatterjee*; Bhartendu Bharti; Kranti Bhavana; Guna Bharathi
Department of ENT, AIIMS, Patna, India.
*Corresponding Author : Chandrani Chatterjee
Department of ENT, AIIMS, Patna, India.
Tel: 8340413441;
Email: drcc87@gmail.com
Received : Dec 04, 2023
Accepted : Dec 29, 2023
Published : Jan 05, 2024
Archived : www.jcimcr.org
Copyright : © Chatterjee C (2024).
Abstract
Non-recurrent laryngeal nerve is a rare anomaly which makes it prone to iatrogenic injury during thyroid surgeries. The aim of this article is to show the presence of non-recurrent laryngeal nerve in a patient being operated for thyroidectomy. A detailed anatomical knowledge and meticulous surgical techniques is a must to ensure its integrity and there is no substitute for the same.
Keywords: Non-recurrent laryngeal nerve; Thyroid surgeries; Anatomical variation; Surgical challenges.
Abbreviations: NRLN: Non-recurrent laryngeal nerve; RLN: Recurrent laryngeal nerve.
Citation: Chatterjee C, Bharti B, Bhavana K, Bharathi G. Non-recurrent laryngeal nerve: An anatomical variation in thyroid surgery. J Clin Images Med Case Rep. 2024; 5(1): 2779.
Introduction
A detailed anatomical knowledge, a meticulous and an organized approach is mandatory before embarking on the journey of thyroid surgeries. Major researches and new technologies have evolved over the last few decades: among those are minimally-invasive thyroidectomies, intra-operative nerve monitoring and new devices for achieving hemostasis and dissection. The essential objectives for thyroidectomy have however always been the avoidance of injury to the nerves, an optimal hemostasis and preservation of parathyroids.
Regarding the identification of Recurrent Laryngeal Nerve (RLN), it is now believed that the “nerve not seen is damaged” rather than “seen is damaged” as was earlier believed. Recurrent laryngeal nerve is a branch of vagus nerve. On right side it loops around subclavian artery and on the left side it loops around aorta to enter the neck on either sides of trachea. Rarely, it can have a non-recurrent course where the nerve without forming a loop enters the larynx behind crico-thyroid joint. Incidence of this rare anatomical variant is around 0.3%-0.8% on the right side and 0.004% on the left side [1]. Intraoperative identification of this anatomical variation and preservation of the nerve can be a challenge even for the most experienced surgeon. We present one such case to emphasize the importance of this variation during thyroid surgery.
Case report
A 23 years old female presented to ENT OPD at AIIMS, Patna with an anterior neck swelling without any clinical features of compression, hypothyroidism or hyperthyroidism. On examination, single 4x3 cm nodule in the right lobe of thyroid was found. Laboratory tests confirmed an euthyroid profile. On Ultrasonography, multiple round to oval well defined nodules with cystic degeneration were noted with TIRADS 3 staging. USG guided FNAC was suggestive of Bethesda Category III -Atypia of Undetermined Significance (AUS).
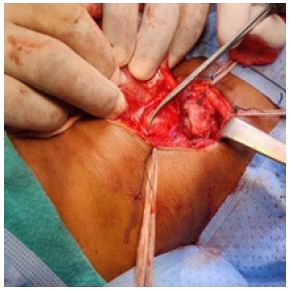
Patient underwent right hemithyroidectomy under general anaesthesia. Careful tissue dissection was performed in the plane between carotid sheath and trachea. The RLN was not identified in its usual anatomical position. A nerve-like structure was identified entering the trachea at the level of cricothyroid joint transversely. On tracing it in a retrograde manner, the nerve was seen arising from vagus nerve. We concluded that it was a non-recurrent laryngeal nerve on right side (Figure 1). Parathyroid glands were preserved. Post-operative period was uneventful. Final Histopathological examination showed colloid goitre with lymphocytic thyroiditis (Figure 1).

Discussion
Non-recurrent laryngeal nerve is a rare embryological anomaly which is often found in conjunction with vascular abnormalities. It was first reported by Stedman in 1823 during cadaveric dissection. He found a “right inferior laryngeal nerve in a non-recurrent situation” associated with a right subclavian artery in an abnormal position behind the oesophagus, and proposed a relationship between the findings [2].
Inferior laryngeal nerve originates from sixth branchial arch. On right side, following the disappearance of fifth and sixth arch, the inferior laryngeal nerve recurs around the fourth arch (i.e. subclavian artery on the right and aortic arch on the left). When the 4th arch disappears as a result of anomalous development the nerve migrates cranially. Thus, it reaches the larynx at a cervical level with a transverse, non-recurrent course. This condition is associated with absent brachiocephalic artery with subsequent origin of the right subclavian artery from the aortic arch distal to the origin of left subclavian artery. Patients with this vascular malformation may experience dysphagia (dysphagia lusoria) due to compression of the oesophagus by retro-oesophageal artery. The NRLN on the left is associated with situs inversus.
NRLN’s are classified as: Type 1: arises directly from vagus nerve and runs together with superior thyroid vessels (Figure 2); Type 2A: parallel transverse path, over the inferior thyroid artery trunk; and Type 2B: parallel transverse path, under the trunk or between the inferior thyroid artery branches [3] (Figure 2). In our case, it is type 1 right non-recurrent laryngeal nerve which was found entering the larynx behind the cricothyroid joint in a transverse path. Recurrent laryngeal nerve was not found in its usual location and with meticulous dissection the NRLN in our patient was preserved.
The NRLN cannot be identified by any pre-operative imaging but the detection of an arterial lusoria may serve as a complimentary indicator of presence of NRLN. Barium swallow might show indentation in the posterior oesophageal wall by an anomalous vessel (the bayonet sign). CT and MR can demonstrate directly the presence of the lusorian artery and the absence of brachiocephalic trunk. Ultrasound is a simple, rapid, non-invasive and cost-effective tool to detect a NRLN. Usually, the right common carotid and the right subclavian artery arise together from the bifurcation of the brachiocephalic artery, describing a Y, which has been termed as “Y-sign” [4]. Absence of “Y-sign” indicates aberrant origin of a subclavian artery.
However routine use of these investigations preoperatively is limited by the variable diagnostic accuracy, invasiveness and costs. The best way to avoid damage to inferior laryngeal nerve in thyroidectomy surgery is to identify the nerve with systematic diligent dissection based on the usual anatomical landmarks and keeping in mind the possibility of an anatomical variation. Liu et al. suggested that any transverse band (with the exception of middle thyroid vein) should not be cut unless the RLN is identified and preserved [5].
Conclusion
Non recurrent laryngeal nerve incidence is very rare but when present, is associated with high risk of iatrogenic injury. Pre-operative radiology might indicate a presence of vascular anomaly in conjunction with NRLN. The bottom line however is that nothing can substitute a detailed anatomical knowledge and a diligent surgical technique. Hence it is mandatory to be aware of non-recurrent laryngeal nerve incidence, course and associated anatomical variations.
Acknowledgement: This is a non-funded, non-supported academic article for which I am grateful to all the participants for their valuable inputs and the Department of ENT at AIIMS, Patna. We would also like to thank the Operating surgeon for providing us with the surgical insight and the Head of Department of ENT at AIIMS, Patna for her guidance in the construction of this article.
References
- Uludag M, Isgor A, Yetkin G, Citzeg B. Anatomic variations of the non-recurrent inferior laryngeal nerve. BMJ Case rep. 2009
- Stedman GW. A singular distribution of the nerves and arteries of the neck and the top of the thorax. Edinb Med Surg J. 1823; 19: 564-5.
- Branscom JJ, Austin JH. Aberrant right subclavian artery. Findings seen on plain chest roentgenograms. Am J Roentgenol Radium Ther Nucl Med. 1973; 119: 539-42.
- Citton M, Giovanni V, Maurizio I. Neck Ultrasonography for detection of non-recurrent laryngeal nerve; Gland surgery. 2016; 5: 583-590
- Liu LX, et al. The importance of nonrecurrent laryngeal nerve in thyroid surgery (in Chinese). Zhonghua Wai Ke Za Zhi. 2006; 44: 904-906.