
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Metastatic pulmonary calcifications secondary to end-stage renal disease
Ujaas Dawar2; Nasir Akhtar1; Muhammad Shafiq1*; Kanwar Pannu2; Johnson Samuel2; Dipak Mukherjee2
1Department of Respiratory Medicine, Hull University Teaching Hospitals NHS Trust, Hull, United Kingdom.
2Department of Respiratory Medicine, Basildon University Hospital, Mid and South Essex NHS Foundation Trust, United Kingdom.
*Corresponding Author : Muhammad Shafiq
Department of Respiratory Medicine, Hull University Teaching Hospitals NHS Trust, Hull, United Kingdom
Email: sheeki82@gmail.com
Received : Dec 04, 2023
Accepted : Dec 29, 2023
Published : Jan 05, 2024
Archived : www.jcimcr.org
Copyright : © Shafiq M (2024).
Abstract
Metastatic Pulmonary Calcification (MPC) is described as the deposition of calcium in normal lung parenchyma and is commonly associated with secondary hyperparathyroidism resulting from end-stage renal disease. The diagnosis of MPC can be determined through a clinical and biochemical assessment of secondary hyperparathyroidism, in conjunction with HRCT findings, without the necessity for a biopsy.
Antemortem diagnosis of MPC is infrequent. Here, we share the case of a middle-aged male with MPC, underscoring the significance of early identification and management of this often-overlooked condition.
Keywords: Kidney failure; Chronic; Hyperparathyroidism secondary; Metastatic pulmonary calcifications; High-resolution CT chest; Early recognition.
Citation: Dawar U, Akhtar N, Shafiq M, Pannu K, Samuel J, et al. Metastatic pulmonary calcifications secondary to end-stage renal disease. J Clin Images Med Case Rep. 2024; 5(1): 2780.
Case description
A male in his early 50s presented with chronic cough and breathlessness. He had been experiencing this cough for the past three to four years, and it was usually productive with clear to yellow phlegm. The cough turned from yellow to green during episodes of chest infection, which required antibiotics. There was no history of associated hemoptysis. He started to become breathless on exertion during the same period, which progressively worsened over a few years to the point where he was breathless on walking from room to room at home. Additionally, the patient reported intermittent episodes of wheezing.
He had developed End-Stage Renal Failure (ESRF) following atypical hemolytic uremic syndrome and was on dialysis for eight years. His other medical history included mitral valve stenosis with calcified vegetation, ischaemic heart disease with coronary artery bypass graft, and Bell’s palsy.
He worked as a racehorse jockey as a young and eventually medically retired as a chef. He was a lifelong tobacco smoker and a recreational user of cocaine in the past. He had no personal history of tuberculosis or known tuberculosis contacts. He had no relevant history of occupational exposure to inhalants, toxins, or fumes.
A review of previous blood tests showed persistently elevated phosphate and PTH levels, with normal calcium, suggesting secondary hyperparathyroidism associated with End-Stage Renal Disease (ESRD). The latest blood tests are shown in Table 1.
Sequential chest X-rays of the same period showed progressive ground glass changes in both lung fields.
A High-Resolution (HR) CT chest showed diffuse lung parenchymal changes with predominantly bilateral upper lobe high-density/calcified spiculated opacities (Figure 1), and along the oblique fissure in the right lower and left lower lobes. Moreover, there were extensive centrilobular ground-glass changes.
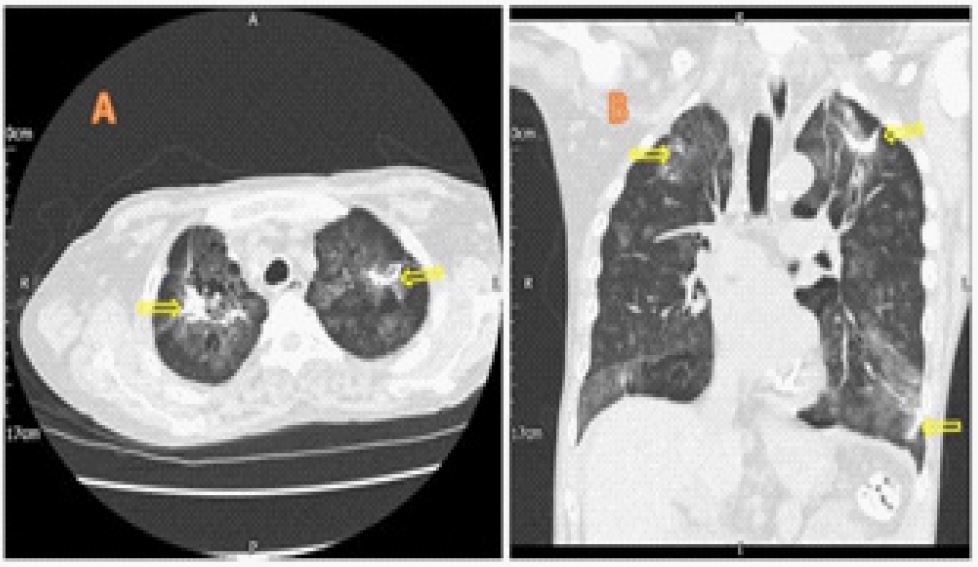
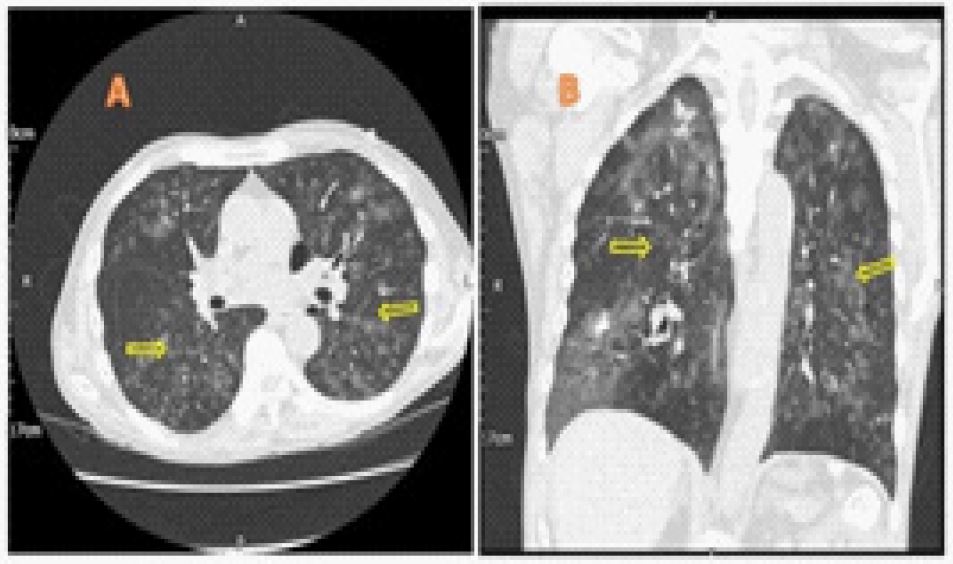
Table 1: Summarising the blood values.
| Test | Result | Reference Range |
|---|---|---|
| Urea | 13.3 mmol/L | 2.5-7.8 mmol/L |
| Creatinine | 632 umol/L | 59-111umol/L |
| ParathyroidHormone (PTH) | 77.9 pmol/L | <9.3 pmol/L |
| Phosphate | 2.74 mmol/L | <1.5 mmol/L |
| Adjusted Calcium | 2.55 mmol/L | <2.6 mmol/L |
Incidental mitral and aortic valve leaflets calcifications were seen. Of note, on the previous CT scan a year ago (Figure 2), these changes were subtly evident but went unrecognised until had significantly progressed.
Lung function test showed a mixed obstructive and restrictive pattern with FEV1 1.38 L (54.6% predicted), FVC 2.30 L (75%), FEV1/FVC 60, TLCO 35% predicted and KCO 48% predicted.
A Bronchoscopy was performed to rule out atypical infections. The bronchial washings cultures grew Escherichia coli & Staphylococcus aureus and tuberculosis and fungal cultures were negative. The cytology showed numerous neutrophils, some lymphocytes and macrophages. No malignant epithelial cells were seen. Bronchoscopy findings were consistent with co-existent bacterial infection requiring antibiotics treatment.
The differential diagnosis of bilateral upper lobe ground glass chronic nodularity is broad, including atypical infections, hypersensitivity pneumonitis, alveolar haemorrhage, sarcoidosis, occupational lung disease, and pulmonary alveolar microlithiasis [1].
Based on clinico-radiological presentation, a diagnosis of Metastatic Pulmonary Calcification (MPC) was concluded in this patient.
Metastatic Pulmonary Calcification (MPC) refers to calcium deposition in the lung parenchyma of normal lungs [2]. MPC has an upper lobe predominance as the lung apex is relatively over-ventilated (high V/Q ratio, 3:1) resulting in low PaCO2 and promoting alkaline environment. Secondary hyperparathyroidism is a common complication of chronic kidney disease and can predispose to metastatic calcifications in relatively alkaline tissues.
Patients are often initially asymptomatic, but may develop progressive lung fibrosis, hypoxia, and respiratory failure [3]. Lung function tests are often normal but can be restrictive with low diffusion capacity due involvement of the alveolar interstitium. In this patient, the flow volume loop pattern was mixed, and gas diffusion was low due to combination of smoking related COPD and parenchymal fibrosis.
HRCT chest is much more sensitive than a chest X-ray in finding small calcifications without the need for an open lung biopsy [4].
Early recognition of this condition and treatment of the underlying cause can help resolve and/or halt progressive lung parenchymal changes.
Treatment should aim to control underlying secondary hyperparathyroidism in end-stage renal disease, in addition to dialysis, with dietary changes, vitamin D supplements, phosphate binders, calcimimetics and some may eventually require parathyroidectomy.
Our patient was treated with non-calcium phosphate binders, 1-alfacalcidol, and cinacalcet to treat secondary hyperparathyroidism, hence resulting in normo-calcemia in the setting of secondary hyperparathyroidism.
Unfortunately, we could not assess the response to treatment as patient was poorly compliant with the prescribed treatment and regular dialysis leading to decline in his general health. He was referred to the local hospice for support and commenced palliative care.
Learning points
• MPC is a benign metabolic lung condition and is a common complication of ESRF resulting in secondary hyperparathyroidism.
• HRCT is very sensitive in diagnosing MPC.
• Early recognition and appropriate treatment is vital to prevent lung fibrosis and respiratory failure.
References
- Walter JM, Stanley M, Singer BD. Metastatic pulmonary calcification and end-stage renal disease. Cleveland Clinic journal of medicine. 2017; 9: 668.
- Chan ED, Morales DV, Welsh CH, et al. Calcium deposition with or without bone formation in the lung. American Journal of Respiratory and Critical Care Medicine. 2002; 165: 1654-69.
- Brodeur Jr FJ, Kazerooni EA. Metastatic pulmonary calcification mimicking air-space disease: Technetium-99m-MDP SPECT imaging. Chest. 1994; 106: 620-2.
- Belém LC, Zanetti G, Souza Jr AS, et al. Metastatic pulmonary calcification: State-of-the-art review focused on imaging findings. Respiratory medicine. 2014; 108: 668-76.