
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Mees’ lines transverse leukonychia
*Corresponding Author : Luis Guillermo Moreno Madrigal
Department of Internal Medicine, Hospital General Regional 1 Dr. Carlos Mac Gregor Sánchez Navarro, Mexican Social Security Institute, Mexico city, Mexico.
Tel: +52-55-54-56-45-67;
Email: rad_marinova@abv.bg
Received : Dec 05, 2023
Accepted : Dec 29, 2023
Published : Jan 05, 2024
Archived : www.jcimcr.org
Copyright : © Moreno Madrigal LG (2024).
Keywords: Nails; Arsenic poisoning; Heart failure; Acute kidney injury.
Citation: Moreno Madrigal LG. Mees’ lines transverse leukonychia. J Clin Images Med Case Rep. 2024; 5(1): 2781.
Case presentation
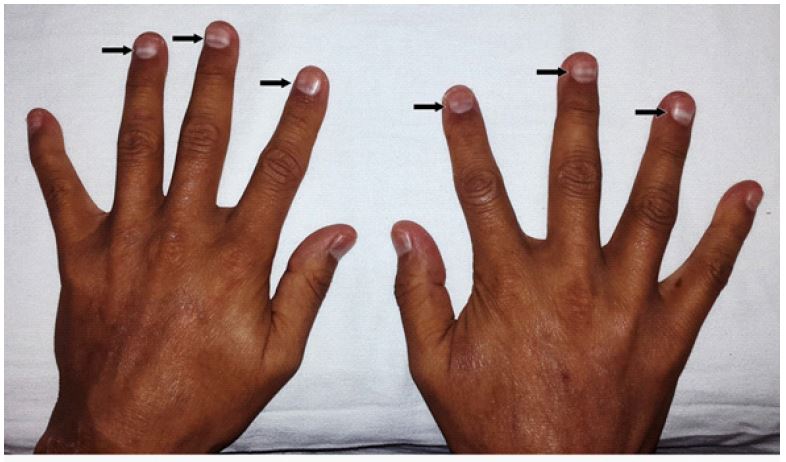
A 56-year-old man was admitted to the hospital for acute decompensated heart failure and acute kidney injury. He had a history of smoking, hypertension, and obesity. He was diagnosed with acute myocardial infarction and received medical treatment. During his stay, he noticed the appearance of transverse, white, 2 mm wide, non-blanchable lines on the nails of all of his fingers and toes, which persisted over the following days and progressively migrated with the growth of the nail (Figures 1 and 2). These findings were compatible with a diagnosis of Mees’ lines.

Discussion
Mees’ lines are also known as transverse leukonychia, Aldrich-Mees’ or Reynolds lines [1-3]. Were first described by Mees in 1919 secondary to arsenic intoxication [1], but they can occur with chemotherapy, paraquat, trauma, renal failure, Hodgkin disease, sickle cell anemia, heart failure and infectious diseases (leprosy, tuberculosis, malaria, herpes zoster, COVID-19) [1,2].
They are resulted from an insult to the nail matrix that can cause transient paraqueratosis of the ventral nail plate without cessation of the nail matrix growth. The lines can present as a retrospective indicator of a pathologic state because their onset is correlated with a systemic insult [2]. Mees’ lines disappear after the causative agent has ceased [1]. The main differential diagnoses are Muehrcke’s lines (they are blanchable and do not migrate with nail growth) and Beau’s lines (which are depressions in the nail plate) [3].
Declarations
Conflicts of interest statement: No conflicts of interest.
Funding: There is no source of funding.
Consent: No identifying markers include as part of medical images. No consent required.
References
- Fernandez-Nieto D, Jimenez-Cauhe J, Dominguez-Santas M. Transverse leukonychia (Mees’ lines) nail alterations in a COVID-19 patient. Dermatologic Therapy. 2020; 33: e13863.
- Lee SH, Kim WH. Mees’ lines associated with heart failure. QJM: An International Journal of Medicine. 2019; 223.
- Sampagar A, Sarapu K, Cheguri S. Mees’ Lines in the Maintenance Phase of Chemotherapy in T‑Lymphoblastic Leukemia. Indian Journal of Pediatrics. 2023.