
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Urethral viral warty (Condyloma acuminatum) lesion presented as urethral tumour: A case report and literature review
Mohamad Homsi Jebrini1*; Layla Zeitouni2; Vishal Mehta3; Waseem Mulhem4; Mohamed Y Hammadeh5
1Oncology Centre, Beatson Hospital, Glasgow, UK.
2Queen Elizabeth University Hospital, Glasgow, UK.
3Histology Department, Lewisham and Greenwich NHS Trust, London, UK.
4Urology Department, Lewisham and Greenwich NHS Trust, London, UK.
5Blackheath Hospital, Circle Health Group, London, UK.
*Corresponding Author : Mohamad Homsi Jebrini
Oncology Centre, Beatson Hospital, Glasgow UK
Email: dr.homsi95@gmail.com
Received : Dec 05, 2023
Accepted : Jan 01, 2024
Published : Jan 08, 2024
Archived : www.jcimcr.org
Copyright : © Homsi Jebrini M (2024).
Abstract
Urethral warts (condyloma acuminatum, CA) frequency is up to 12.5% of genital warts cases [1]. This case study reports a 78-year-old patient with a known history of penile shaft warts presenting with new onset haematuria. Flexible cystoscopy revealed papillary looking tumours in the bulbar urethra suspicious of primary urethral cancer. Tumour biopsy and subsequently excision confirmed CA with moderate dysplasia on biopsy. Patient considered for regular endoscopy follow up.
Keywords: Genital warts; Urethral warts; Urethral cancer.
Citation: Homsi Jebrini M, Zeitouni L, Mehta V, Mulhem W, Hammadeh MY. Urethral viral warty (Condyloma acuminatum) lesion presented as urethral tumour: A case report and literature review. J Clin Images Med Case Rep. 2024; 5(1): 2782.
Introduction
Condylomata Acuminata (CA) or genital warts are common sexually transmitted infections worldwide. They pose a significant burden to healthcare facilities due to rates of transmission and challenges in clearing the underlying infection. Genital warts also pose a psychological burden on patients due to the stigma associated with the infection. Genital warts are caused by Human Papilloma Virus (HPV). HPV strains are divided into low, intermediate, and high risk depending on the probability of dysplasia and ensuing oncogenic change. We present an uncommon case of urethral condyloma acuminatum.
Case description
A 78-year-old male presented with gross haematuria. He has a longstanding history of penile shaft skin warts which worsened over the past 5 years, despite treatment with topical agent and cryotherapy. Previous urological history includes a bulbar urethral stricture, treated with optical urethrotomy and TURP with benign histology. There is no history of UTIs or skin conditions. He is an ex-smoker and has had regular sexual partners.
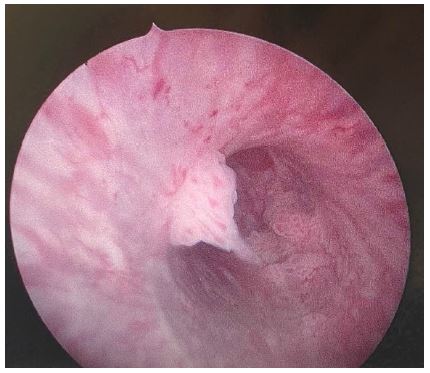
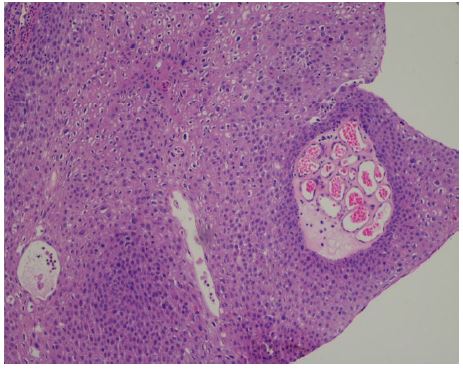
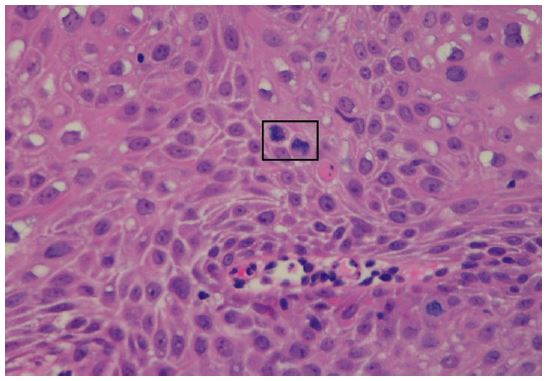
CT intravenous urogram showed normal upper tracts and bladder and flexible cystoscopy showed multiple papillary looking tumours in the bulbar urethra (Figure 1). Subsequent biopsy of urethral tumours confirmed Condyloma Acuminatum (CA) with moderate dysplasia (Figures 2 & 3). P16 immunostaining, which is the surrogate marker for high-risk HPV infection, was negative although the possibility of low-risk HPV infection cannot be excluded.
He was referred to our regional penile cancer centre and he had GA cystoscopy, and the penile and bulbar urethral warts were excised and histology again confirmed CA with moderate dysplasia. He was discussed in the regional MDT and the advice was to have regular flexible cystoscopy every 4-6 months.
Discussion
CA (Genital warts) are common genital problems, mostly caused by Human Papillomaviruses (HPV) [2] of which there are more than 100 strains. Clinical presentation is variable and usually presents as flesh-coloured growths with an irregular surface. Areas infected in men include the perianal and periurethral region, scrotum, and penile shaft. In women, the vulva, vagina, cervix, and perianal region may be affected. CA may also occur in the mouth or throat following oral sexual contact [3]. The incubation period ranges between three weeks to eight months with symptoms manifesting 2-3 months after sexual contact.
The frequency of Urethral CA, such as in our case, is up to 12.5% of genital warts cases [1]. Clinical presentation includes haematuria, coital bleeding, or urinary obstruction. An important differential to exclude is a primary urethral carcinoma.
Infection with high-risk HPV 16 and 18 serotypes has been associated with cervical cancer, oropharyngeal tumours and anal carcinoma. The association of HPV infection with urethral dysplasia, like in our case, and urethral carcinoma is not well established in the literature.
Zhang et al proposed a new type of primary urethral carcinoma that develops in association with HPV infection. From a pool of 106 patients (73 males, 33 females) with primary urethral carcinoma, 31.6% of the tumours had evidence of high-risk HPV infection [4]. Furuhata et al presented a case of severe dysplasia of a urethral CA associated with HPV 11 infection [5].
Treatment of genital warts is challenging. Some cases may resolve without any therapy through immune mediated activated lymphocytes. However, most medical treatments cater to removing the warts rather than eliminating the underlying infection. Unfortunately, this means that recurrence is likely. Our patient has struggled with their recurrence following multiple topical agents, cryotherapy, and diathermy.
Currently, there are no guidelines regarding the management of urethral warts. Usual topical treatments such as Imiquimod cannot be used due to effects on the urethral mucosa.
Techniques such as cryotherapy may not be applicable due to difficult access to the urethra. Surgical transurethral resection, like in our case, may be carried out but carries the risk of fibrosis and consequently, urethral stricture. In atypical and persistent cases, repeat biopsies are recommended to rule out malignancy despite treatment [1].
Follow up of genital warts depends on their location, severity and treatment provided. The consensus for medical treatments is three to six months follow up to monitor for recurrence. Follow-up for patients who had undergone excision and reconstruction is dependent on the procedure performed. In our case, the patient will require regular flexible cystoscopy under local anaesthesia to monitor for potential recurrence of his urethral warts or malignant changes.
The introduction of the quadrivalent HPV vaccine as a prophylactic measure has resulted in significant reduction in external genital warts in both men and women [2]. However, these vaccines are prophylactic and not therapeutic and cannot eradicate an underlying HPV infection.
Conclusion
Genital warts pose a significant financial burden on healthcare and psychological burden on patients. The challenge lies with available management only removing active warts rather than eradicating the causative HPV infection. The preventative HPV vaccine has proven to be 99% effective in preventing genital warts in previously uninfected patients [3] however its role is restricted to prevention rather than treatment. Follow-up is important to check for recurrence and will vary depending on presentation, severity and location.
References
- Florin H, Snoeck R, Van Cleynenbreugel B, Albersen M. Treatment of intraurethral condylomata acuminata with surgery and cidofovir instillations in two immunocompromised patients and review of the literature. Antiviral Research. 2018; 158: 238-243.
- Steben M, M Garland S. Genital Warts. Best Practice & Research Clinical Obstetrics Gynaecology. 2014; 28.
- Yanofsky VR, Patel RV, Goldenberg G. Genital warts: A comprehensive review. J Clin Aesthet Dermatol. 2012; 5: 25-36.
- Zhang M, Adeniran AJ, Vikram R, Tamboli P, Pettaway C, et al. Carcinoma of the urethra. Hum Pathol. 2018; 72: 35-44.
- Furuhata M, Fujimoto Y, Nukui F, Nagata M, Okamoto S, et al. Urethral condyloma acuminatum with severe dysplasia in a male patient detected human papillomavirus type 11: A case report. Hinyokika Kiyo. 1993; 39: 857-61.