
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Granulicatella elegans infective endocarditis, a rare case report at a secondary teaching hospital, Tangerang, Indonesia
Veronica Wiwing1*; Ivani Christina Kurniadi2; Hendyono Lim3; Neneng Suryadinata4; Cucunawangsih Cucunawangsih1
1Department of Microbiology, Faculty of Medicine, University of Pelita Harapan, Tangerang, Indonesia.
2Faculty of Medicine, University of Pelita Harapan, Tangerang, Indonesia.
3Department of Cardiology, Faculty of Medicine, University of Pelita Harapan, Tangerang, Indonesia.
4Department of Histology, Faculty of Medicine, University of Pelita Harapan, Tangerang, Indonesia.
*Corresponding Author : Veronica Wiwing
Department of Microbiology, Faculty of Medicine, University of Pelita Harapan, Tangerang, Indonesia.
Email: veronica.wiwing@uph.edu
Received : Dec 08, 2023
Accepted : Jan 01, 2024
Published : Jan 08, 2024
Archived : www.jcimcr.org
Copyright : © Wiwing V (2024).
Abstract
Granulicatella elegans (G. elegans) is a Gram-positive facultative anaerobe and one type of Nutritionally Variant Streptococci (NVS) normally role as normal flora in human body, for example oral cavity. Rarely had this colony become infective compared to other Granulicatella. Considering the difficulty in growing of this organism on culture media, as well as the fact that this organism could be one of the bacteria responsible for infective endocarditis suggests that its pathogenic role may be underestimated. G. elegans being considered a rare causative agent and not a target of standard empiric antibiotic treatment. Therefore, once this organism appears as a pathogen especially in infective endocarditis, it becomes a challenge on how to manage the patient’s treatment to reduce the mortality risk. We present a rare case of G. elegans infective endocarditis with the aim of sharing knowledge about this microorganism, which can be challenging for physicians unfamiliar with it.
Citation: Wiwing V, Kurniadi IC, Lim H, Suryadinata N, Cucunawangsih C. Granulicatella elegans infective endocarditis, a rare case report at a secondary teaching hospital, Tangerang, Indonesia. J Clin Images Med Case Rep. 2024; 5(1): 2784.
Introduction
Infective Endocarditis (IE) is an uncommon medical condition which has a high mortality rate (10-30%) among patients. There are several risk factors which may initiate the conditions such as degenerative valve sclerosis, intravenous drugs exposure, intracardiac device, and invasive medical procedures [1,2]. G. elegans considered as one of NVSs which require pyridoxal, cystine or helper bacteria such as staphylococci to adequate grow. The NVSs have been divided into two genera, Abiotophia and Granulicatella. As commensal microbiota of mouth, upper respiratory, urogenital, and gastrointestinal tract, G. elegans were recorded in 5-6% case of IE [3,4]. Isolation of this bacterium is difficult, and its role as a cause of infection is likely underestimated since some cases of culture-negative endocarditis might be caused by this microorganism. It has been noted to be less infectious than the other granulicatella due to low binding capacity to extracellular matrix protein, yet it might be present in 10% cases of adult infective dental plaque [5-7]. Thought it is rare, we present a case of endocarditis due to Gelegan.
Case presentation
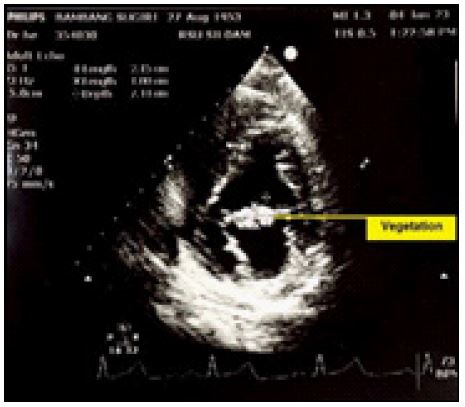
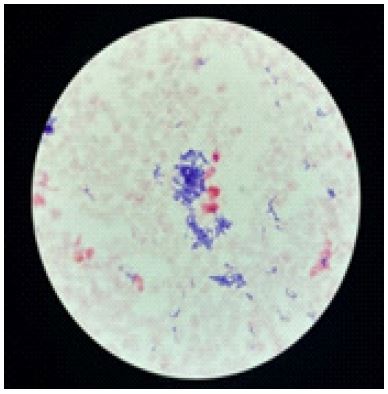
A 69-year-old male came to Cardiology Department with a symptoms of mild chest pain which lasted 1 week before appointment without fever. He had history of hypertension, cardiovascular disease, and Parkinson on treatment. The echocardiography (Figure 1) showed a vegetation at Anterior Mitral Leaflet (AML) which cause severe mitral regurgitation. Hospital admission was then required with suspect of infective endocarditis. His blood test results were as follows, haemoglobin 10.50 g/dL, haematocrit 33.10%, white blood cell 14.030 μL, Erythrocyte Sedimentation Rate (ESR) 55 mm/hours, with stool occult blood positive. The remainder laboratory result, including serum biochemistry, coagulation tests, rheumatoid factors, antinuclear antibody, immunoglobulin, and urine analysis were within normal. As further examination, blood cultures was later taken for 3 serial specimens, which showed Granulicatella elegans (Figures 2 & 3) as the causative agent, originally as the normal-flora oral mucous. Automated system VITEX 2 indicated that the bacteria was sensitive to various antibiotics such as gentamicin, amoxicillin/clavulanic acid, cefotaxime, ceftriaxone, vancomycin, clindamycin, and ampicillin. Meanwhile, it was resistant to metronidazole and kanamycin by disc diffusion method in chocolate agar and incubation in 10% CO2. Numerous dental caries found on oral examination which likely confirm the diagnosis. Odontectomy of 11 teeth towards the patient were performed to evacuate possible source of infection and prevent bacteraemia. Panoramic imaging was impracticable since the patient could not be positioned vertically. According to susceptibility result, ceftriaxone 2 grams daily combined with gentamicin 1 mg/kg IV q8h were chosen as the definitive therapy of this disease for 6 weeks ahead. Repeat blood culture 72 hours after initiation of antibiotic treatment were negative. The patient clinically improved without any evidence of relapse after his discharge from the hospital.

Discussion
Granulicatella elegans is a rare microorganism causing infective endocarditis compared to other Granulicatella species, that are G. adiacens and G. balaenopterae; these were previously included in the genus Abiotrophia. Isolation of this organisms is difficult, as it requires pyridoxal or active vitamin B6 to grow. This vitamin has responsible for co-enzymatic transformation of l-alanine to d-alanine, which required for peptidoglycan production. In this case, we isolated the bacteria only on chocolate agar which contain a small amount of pyridoxal from haemolyzed red blood cells.
These organisms not only from form part of normal flora, but also cause infections such as abscess, conjunctivitis, endophthalmitis, glomerulonephritis, and sepsis. Its bacteraemia progress usually initiates from oral cavity and shows large cardiac vegetation (>10 mm) [5]. The most frequent valves involved are aortic (44%) then mitral (38%) valve [6]. Duke Criteria is commonly used to point the disease, divided into Major Criteria’s and Minor Criteria’s. The Major consists of blood culture positive and endocardiographic evidence of endocardial involvement, meanwhile the minor consists of temperature of 38°C; immunological phenomenon; microbiological evidence; embolic phenomenon; and risk factor of heart disorders [2]. IE is defined when there are 2 major criteria’s or 1 major + 3 minors or 5 minors. It is possible to be diagnosed as IE when there are 1 major + 1 minor or 3 minor criterions. Other important examination such as blood laboratory check and culture are needed to determine the treatment. In this patient, we found that 2 major criteria which make the diagnosis definite.
Further follow-up is needed to monitor the patient’s progress. This nutrient variant streptococcus results a challenging treatment due to poor outcome and high mortality rate [7,8]. Cardiac surgery is an option for those who have severe valve damage. On the other hand, the surgery should be postponed based on guideline, as the patients have previous medical condition such as anemia, melena, and chronic neurological complications [9].
Long-term combination therapy with β-lactam antibiotics and aminoglycosides is recommended, and also vancomycin is an effective regimen for resistant strains. In vitro, this bacterium shows susceptibility to various type of β-lactam, gentamicin, vancomycin, meropenem, and clindamycin. rifampicin, ofloxacin, levofloxacin, and quinupristin-dalfopristin [2]. Regardless of in vitro results, treatment failure occurs in approximately 41% of cases, and nearly 27% require prosthetic valve replacement, mainly due to congestive heart failure or large systemic embolism [10].
Conclusion
Granulicatella elegans is a normal flora of oral cavity which able to transform into opportunist in causing infective endocarditis due to patients underlying conditions. The condition does not always require a surgical treatment unless there are several life-threatening aspects such as embolism and large/multiple vegetations, according to the guidelines.
Declarations
Conflicts of interest: The authors declare no interest.
Informed consent: Written informed consent was obtained from the patient for publication and a copy of the consent is available for review on request.
Funding: None.
Acknowledgement: Concept and design: All authors; Drafting of the manuscript: ICK, NS, HL; Critical revision for important intellectual content: All authors; and supervision by HL and CC.
References
- Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, et al. Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). European Heart Journal. 2015; 36: 3075-128.
- Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the management of patients with valvular heart disease: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2021; 77: 197.
- TS Shailaja, KA Sathiavathy, Govindan Unni. Infective endocarditis caused by Granulicatella adiacens, Indian Heart Journal. 2013; 65: 447-449.
- Quartermain L, Tailor H, Njenga S, Bhattacharjee P, Rao GG. Neonatal Granulicatella elegans Bacteremia, London, UK. Emerging Infectious Diseases. 2013; 19: 1165-1166.
- Perera Y, Galagedara W, Gunasekara S, Wijekoon, Sanjeewa, et al. Granulicatella elegans: A rare cause of infective endocarditis A Case Report. Sri Lankan Journal of Infectious Diseases. 2021.
- Adam EL, Siciliano RF, Gualandro DM, Calderaro D, Issa VS, et al. Case series of infective endocarditis caused by Granulicatella species. International Journal of Infectious Diseases. 2015; 31: 56-58.
- Patri S, Agrawal Y Granulicatella elegans endocarditis: A diagnostic and therapeutic challenge. Case Reports. 2016; 2016: bcr2015213987.
- Pettersson GB, Hussain ST Current AATS guidelines on surgical treatment of infective endocarditis. Ann Cardiothorac Surg. 2019; 8: 630-644.
- Albano C, Bagarello S, Giordano S, Sanfilippo MF, Comparato C, et al. Granulicatella spp, a Causative Agent of Infective Endocarditis in Children. 2019 ;8: 630-644.
- Wang A, Fosbøl EL. Current recommendations, and uncertainties for surgical treatment of infective endocarditis: A comparison of American and European cardiovascular guidelines, European Heart Journal. 2022; 43: 1617-25.
- Perkins A, Osorio S, Serrano M, del Ray MC, Sarriá C, et al. A case of endocarditis due to Granulicatella adiacens. Clinical Microbiology and Infection. 2003; 9: 576-577.