
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Superior mesenteric artery syndrome: A case report
Tien Tran Phung Dung; Trung Lam Viet; Lam Nguyen Truong Truc; Huy Nguyen Khac; Huan Nguyen Ngoc*
Digestive Surgery Department, Cho Ray Hospital, Vietnam.
*Corresponding Author : Huan Nguyen Ngoc
Digestive Surgery Department, Cho Ray Hospital, Vietnam.
Email: ngochuan1710@gmail.com
Received : Dec 13, 2023
Accepted : Jan 02, 2024
Published : Jan 09, 2024
Archived : www.jcimcr.org
Copyright : © Nguyen Ngoc H (2024).
Abstract
Superior Mesenteric Artery (SMA) syndrome, also known as Wilkie’s syndrome, is a rare condition of duodenal obstruction due to extrinsic compression of the third portion of the duodenum by the superior mesenteric artery and the abdominal aorta. The syndrome involves small bowel obstruction resulting from compression at the proximal duodenum, but the nonspecific abdominal findings often make this diagnosis initially difficult. We report a case of a 19-year-old female who had chronic upper abdominal pain of unknown origin, which was later confirmed as SMA Syndrome and referred for surgical treatment. SMA syndrome should be suspected in a young female who presents with nonspecific abdominal symptoms, rapid weight loss, and functional dyspepsia, as well as nausea, vomiting, and inconclusive laboratory and physical exam findings. Early treatment is essential to prevent serious complications from worsening. SMA syndrome is a very rare condition and usually a diagnosis of exclusion, so many other more common conditions need to be ruled out first. The laparoscopic approach is preferred over the open approach, as it has fewer postoperative complications and faster recovery.
Keywords: Wilkie syndrome; Superior mesenteric artery syndrome; Aorto-mesenteric compass syndrome.
Citation: Nguyen Ngoc H, Phung Dung TT, Lam Viet T, Truong Truc LN, Nguyen Khac H. Superior Mesenteric Artery Syndrome: A Case Report. J Clin Images Med Case Rep. 2024; 5(1): 2787.
Introduction
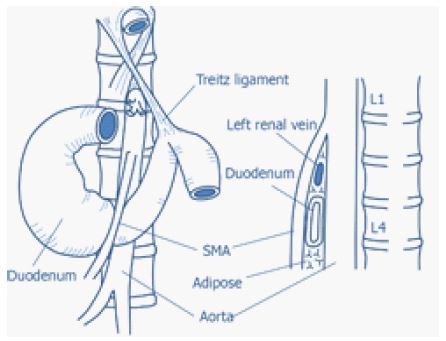
SMA syndrome, also known as Wilkie’s syndrome, is a rare disorder that occurs when the SMA and the abdominal aorta squeeze the third portion of the duodenum. It has a low incidence of about 0.1-0.3% and affects women more than men [1]. Chronic epigastric abdominal pain, nausea and vomiting after eating, and rapid weight loss in the recent past are the main clinical manifestations of superior mesenteric artery syndrome [2]. The condition is diagnosed by combining clinical and imaging evidence, usually involving a contrast-enhanced upper GI study and an abdominal CT scan. The diagnosis of the condition requires a thorough medical history and physical examination. A contrast-enhanced abdominal CT scan is performed to verify the diagnosis by measuring the narrowing of the angle between the aorta and the superior mesenteric artery, which causes the compression of the third part of the duodenum (Figure 1). In addition, one of the characteristic signs of superior mesenteric artery syndrome in upper GI contrast studies is the sudden vertical or oblique compression of the duodenum. The condition can be managed either conservatively or surgically. Surgery is indicated when medical treatment fails to improve the symptoms.
Case presentation
The case of a 19-year-old female with recurrent vomiting, chronic upper abdominal pain, and weight loss for over a year is reported. She had multiple gastric endoscopies and was diagnosed with gastritis, but her symptoms persisted despite medication and follow-ups. The patient had a history of chronic abdominal pain and weight loss. Her physical examination revealed a low body weight (44 kg) and height (170 cm), resulting in a Body Mass Index (BMI) of 16 kg/m2, which indicated severe underweight. Her blood biochemistry tests were within normal ranges and no abnormalities were detected by ultrasound imaging. To confirm the diagnosis and rule out any gastrointestinal abnormalities, the patient underwent upper GI contrast and computer tomography studies. The upper GI contrast study revealed a midline compression of the third portion of the duodenum, which was displaced to the left of the midline (red arrow). The study also showed a mild delay of contrast passage with retrograde peristalsis, but no evidence of duodenal dilation (Figure 2).

The patient also underwent a contrast-enhanced abdominal CT scan for further evaluation. The scan revealed a decreased amount of retroperitoneal fat, which normally separates the upper border of the duodenum and the lower surface of the superior mesenteric artery. This finding suggested a loss of the normal protective cushioning between these structures (Figure 3). The aortomesenteric angle, which measures the degree of compression of the third portion of the duodenum by the aorta and the superior mesenteric artery, was 14° in this case. The aortomesenteric distance, which indicates the gap between these two vessels, was 8 mm. These values confirmed the presence of aortomesenteric compression syndrome (Figure 4).
The patient was advised to undergo surgery after the diagnosis was established. A laparoscopic Roux-en-Y duodenojejunostomy was performed to bypass the compressed segment of the duodenum. The duration of the surgery was 180 minutes. The patient had a smooth postoperative course with no complications and was able to tolerate oral feeding. She was discharged on the fifth postoperative day.


Discussion
The anatomical description of SMA syndrome was first reported by Carl Freiherr Von Rokitansky, an Australian, in 1861 as a post-mortem finding. However, it was not until 1927 that Willkie demonstrated the exact pathophysiology and management of this condition [5]. SMA syndrome is a rare condition that requires better understanding of its risk factors and clinical manifestations. This would enable faster diagnosis and optimal treatment strategy for this disorder. The patient may experience chronic or intermittent nausea, vomiting, and abdominal pain in the upper region after eating, depending on the degree of obstruction. Other symptoms may include feeling full quickly, losing weight rapidly, and having a swollen abdomen. The diagnosis of superior mesenteric artery syndrome is mainly based on two imaging tests: Computed tomography and upper GI contrast. These tests can visualize the external compression of the duodenum and measure the aortomesenteric angle and distance, which are the key indicators of this condition. Endoscopy can also be used to diagnose this condition, but it may fail to detect it if the duodenum D3 is not reached by the scope. Radiography can measure the angle and the distance between the abdominal aorta and SMA, which are the main criteria for this condition. Normally, the aortomesenteric angle ranges from 25° to 60° and the aortomesenteric distance is about 10-20 mm. However, in SMA syndrome, the angle is reduced to 7°-22° and the distance is less than 8 mm [6]. The patient had a reduced aortomesenteric angle of 14° and a decreased aortomesenteric distance of 8 mm (Figure 4), which caused the symptoms. Upper GI contrast was used to show a proximal obstruction with or without gastric dilation and a delayed transit time with a resolution of obstruction in prone knee-chest or left lateral positioning [7]. SMA syndrome is a challenging diagnosis because it has non-specific symptoms and may not show any abnormalities in basic tests. It is a rare condition, but it should be considered as a possible cause of chronic abdominal pain and weight loss. If not diagnosed and treated properly, it can lead to complications such as electrolyte imbalance, malnutrition, and gastroesophageal reflux. In our case, the patient was initially misdiagnosed with gastritis and suffered from delayed treatment. Therefore, Patients with risk factors and no clear cause of upper abdominal pain and vomiting episodes should be evaluated for SMA syndrome. This condition can cause serious complications such as electrolyte imbalance, nutritional deficiency and catabolism, gastric perforation, and peritonitis if not diagnosed and treated timely [8]. The treatment of superior mesenteric artery syndrome requires a combination of conservative and surgical approaches. All patients should receive initial conservative treatment, such as parenteral nutrition, gastric decompression, and proper positioning of the patient after eating. If conservative treatment fails, surgery should be performed as soon as possible. The preferred surgical procedure is duodenojejunostomy, which has a high success rate of around 90% [7]. Laparoscopic duodenojejunostomy is a preferred and widely used technique that reduces the invasiveness of surgery. Our patient underwent this procedure and had a good outcome.
Conclusion
Superior mesenteric artery syndrome is a rare and challenging condition that can be misdiagnosed with other internal diseases. The condition can be life-threatening for the patient due to rapid weight loss and vomiting. Early recognition of risk factors and adequate preoperative nutritional support are essential to prevent serious complications. The laparoscopic approach is preferred over the open one as it has fewer postoperative complications and faster recovery.
References
- Shiu JR, Chao HC, Luo CC, et al. Clinical and nutritional outcomes in children with idiopathic superior mesenteric artery syndrome. J Pediatr Gastroenterol Nutr. 2010; 51: 177-182.
- Rabie ME, Ogunbiyi O, Al Qahtani AS, et al. Superior mesenteric artery syndrome: Clinical and Radiological considerations. Surg Res Pract. 2015; 2015: 628705.
- Oka A, Awoniyi M, Hasegawa N, Yoshida Y, Tobita H, et al. Superior mesenteric artery syndrome: Diagnosis and management. World J Clin Cases. 2023; 11: 3369-3384.
- Von Rokitansky C. Lehrbuch der pathologischen anatomie. Leipzig: Wilhelm Braunmüller. 1855.
- Wilkie D. Chronic duodenal ileus. Br Med J. 1921: 793-795.
- Al Faqeeh AA, Syed MK, Ammar M, Almas T, Syed S. Wilkie’s Syndrome as a Rare Cause of Duodenal Obstruction: Perspicacity Is in the Radiological Details. Cureus. 2020; 12: 10467.
- Mandarry M, Zhao L, Zhang C, et al. A comprehensive review of superior mesenteric artery syndrome. Eur Surg. 2010; 5: 229-236.
- Zaraket V, Deeb L. Wilkie’s syndrome or superior mesenteric artery syndrome: Fact or fantasy. Case Rep Gastroenterol. 2015; 9: 194-199.
- Danushka PGN, Jayasinghe R, Wijemanne A. Superior mesenteric artery syndrome treatment strategies: A case report. SAGE Open Med Case Rep. 2023.