
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Commentary - Open Access, Volume 5
The potential protective role of lactate in the early onset of intensive care unit-acquired weakness (ICU-AW) in patients with shock
Ling Wang*; Dengyan Long
Department of Intensive Care Unit, People’s Hospital of Qiandongnan Miao and Dong Autonomous Prefecture, Kaili City, Guizhou Province, China.
*Corresponding Author : Ling Wang
Department of Intensive Care Unit, People’s Hospital of Qiandongnan Miao and Dong Autonomous Prefecture, Kaili City, Guizhou Province, China.
Email: 463082910@qq.com
Received : Dec 11, 2023
Accepted : Jan 03, 2024
Published : Jan 10, 2024
Archived : www.jcimcr.org
Copyright : © Wang L (2024).
Abstract
The objective was to investigate the correlation between early lactate levels and the early development of Intensive Care Unit-Acquired Weakness (ICU-AW) in patients with septic shock. Data from pneumonia-induced septic shock patients in our ICU were analyzed, dividing them into ICU-AW and non-ICU-AW groups based on ICU-AW development within 7 days. Key parameters like gender, age, and lactate levels at admission and after six hours were compared. The study found no significant differences in gender and age between the groups, but the non-ICU-AW group had higher lactate levels initially and after six hours. The results suggested an inverse correlation between early lactate levels and ICU-AW, indicating that mildly elevated lactate might protect against early ICU-AW in septic shock patients.
Keywords: Septic shock; Lactate; ICU-acquired weakness; Protective role; Muscle; Nerve.
Citation: Wang L, Long D. The potential protective role of lactate in the early onset of Intensive Care Unit-Acquired Weakness (ICU-AW) in patients with shock. J Clin Images Med Case Rep. 2024; 5(1): 2788.
Introduction
Patients with septic shock are commonly admitted to the Intensive Care Unit (ICU) due to the severity of their condition. However, factors such as prolonged hospitalization, limited mobility, mechanical ventilation, and sedative medications can lead to the development of ICUt-Acquired Weakness (ICU-AW), a frequent complication in ICU patients [1,2]. ICU-AW is characterized by a significant decline in symmetrical muscle strength, severely affecting patient prognosis and quality of life [3].
Current understanding of the pathogenesis of ICU-AW primarily involves neurogenic and/or myogenic damage. Lactate is the end-product of anaerobic glycolysis. Some studies suggested that lactate can inhibit mitochondrial function, thereby reducing hypoxic damage to neural cells, aiding in the protection and repair of these cells [4,5]. Additionally, lactate can elevate antioxidant levels, helping to mitigate oxidative damage to cells [6,7], and it may had a protective effect on skeletal muscle strength [8,9]. Based on these findings, we hypothesized that lactate may play a protective role in preventing the occurrence of ICU-AW. Thus, the objective of this study was to investigate the correlation between early lactate levels and the early development of ICU-AW in shock patients.
Materials and methods
Data sources: We selected patients admitted to the comprehensive ICU at Qiandongnan People’s Hospital of Qiandongnan Miao and Dong Autonomous Prefecture between January 1, 2022, and June 8, 2023. Inclusion criteria comprised individuals aged over 18 years with a confirmed diagnosis of septic shock due to pneumonia. We excluded cases with myasthenia gravis, severe central nervous system diseases, various fractures, polymyositis, and other conditions that could affect the diagnosis of ICU-AW, as well as patients with incomplete data or those who had withdrawn from treatment.
Diagnostic criteria: The diagnosis of sepsis met the Sepsis-3 criteria [10], where the need for vasopressors to maintain a mean arterial pressure of over 65 mmHg after adequate fluid resuscitation was considered as septic shock. The diagnosis of ICU-AW was determined using the Medical Research Council (MRC) scale for muscle strength grading in the upper and lower limbs, with patients scoring less than 48 being diagnosed with ICU-AW [1].
Treatment methods: All admitted patients received treatment protocols designed according to the etiology, along with necessary organ support measures to maintain vital sign stability. Patients with hypovolemia underwented adequate fluid resuscitation, and those with infections received effective antibiotic therapy. When necessary, mechanical ventilation, continuous renal replacement therapy, transfusion, and nutritional support were implemented as per requirement.
Study methods: We collected a 3 ml venous blood sample from patients upon ICU admission and measured blood lactate levels using the ABL800 blood gas analyzer from Radiometer, Denmark. Subsequent assessments of blood lactate levels were performed 6 hours later (6h-lactate), and daily measured limb muscle strength to diagnose the ICU-AW. On day 7th, patients were categorized into the ICU-AW and non-ICU-AW groups depending on the development of ICU-AW during their ICU stay, and we compiled data on gender, age, initial lactate, and 6h-lactate for comparison between the two groups.
Statistical methods: Data was analyzed using SPSS software version 26.0. For metric data, the Kolmogorov-Smirnov test was employed to verify normality. Normally distributed metric data was expressed as mean ± standard deviation (x±s), and comparisons between groups were performed using independent sample T-tests. For non-normally distributed metric data, the median (interquartile range) (M (QL, QU)) was used, and group comparisons was made using the Mann-Whitney U test. For count data, the χ2 test was used. A P-value of < 0.05 was considered statistically significant.
Results
A total of 500 patients were included in the study, consisting of 310 males and 190 females. The age range was from 18 to 94 years, with an average age of 63.86 years. The mean duration of shock was 5.09 days, while the average ICU stay was 9.63 days. The ICU-AW group included 216 patients, and the non-ICU-AW group consisted of 284 patients, with an incidence rate of ICU-AW being 44.8%. Over the following three months, a total of 97 patients died, while 403 patients survived.
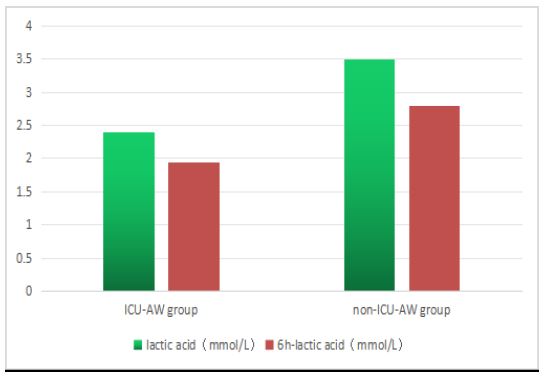
There were no significant differences between the two groups in terms of gender and age (χ2=2.268, t=1.292, all P>0.05). However, the non-ICU-AW group exhibited significantly higher levels of Initial lactate and 6-hour lactate than the ICU-AW group, with values of 3.5 vs. 2.4 and 2.8 vs. 1.95, respectively (Z=-4.530, -4.244, all P<0.05), indicating statistically significant differences. Detailed data were presented in Table 1 and Figure 1.
Table 1: Magnetic resonance of Cholangio
| Parameter | ICU-AW Group (n=216) | Non-ICU-AW Group(n=284) | X2/t/Z | P vilue |
|---|---|---|---|---|
| Gender (Male/Female) | 142/74 | 168/116 | 2.268 | 0.079 |
| Age (Year) | 65.05±18.12 | 62.95±17.80 | 1.292 | 0.197 |
| Initial lactate(mmol/L) | 2.40(1.,0,4.10) | 3.50(1.90,6.58) | -4.530 | 0.000 |
| 6h-lactate (mmol/L) | 1.95(1.30,3.40) | 2.80(1.50,6.52) | -4.244 | 0.000 |
Discussion
The findings of our study indicated that within 7 days, the non-ICU-AW group exhibited marginally higher levels of initial lactate and 6h-lactate (3.5 vs. 2.4 and 2.8 vs. 1.95, respectively) compared to the ICU-AW group, suggested a significant correlation between lactate levels and the incidence of ICU-AW. Consequently, we hypothesized that a slight elevation in lactate levels may confer a protective effect against the early development of ICU-AW in septic shock patients. This discovery contributed to a deeper understanding of the role of lactic acid in this disease.
Lactate has a long time been regarded as a critical indicator of tissue perfusion and systemic oxygen metabolism in patients with shock [11,12], often associated with increased mortality rates and poor prognoses [13-15]. Emerging research suggested that lactate possesses multiple biological activities. It can facilitate muscle mass increment and repair and serve as an energy substrate for neuronal cells, helping to maintain neuronal function and prevent damage [16-18].
We reviewed some studies on the protective effects of lactate on nerve and muscle function. Research had shown that lactate can enter neuronal cells, mitigate hypoxic damage to the brain by inhibiting mitochondrial function, thereby prolonging neuronal survival under hypoxic conditions [19]. Additionally, lactate can protect neurons from injury by increasing VEGF protein expression [20]. Studies also suggested that lactate promotes growth and regeneration in skeletal muscle tissues and cultured cells [18,21], particularly in damaged muscle tissue. One study found that lactate induces muscle growth correlated with an increased number of Pax7 positive nuclei in mouse anterior tibial muscle, suggested a stimulatory effect of lactate on muscle growth and regeneration, especially in damaged muscle tissues [22]. The lactate shuttle hypothesis posited that lactate, as an energy substrate, was exchanged among different tissues, cells, and intracellular compartments, including nerve and muscle tissues [23]. These findings implyed that lactate may play a more complex role within the organism, not merely as a byproduct of energy metabolism but also potentially in intercellular communication, muscle mass maintenance, and regeneration.
Our results speculated that a slight increase in lactate levels may have a protective role during the early development of ICU-AW in septic shock patients, offered new insights and strategies for the prevention and treatment of ICU-AW. However, the exact mechanisms was remain unclear. We proposed that during the early stages of shock, when microcirculatory disturbances lead to tissue hypoxia, lactate could serve as an alternative substrate, providing support even when energy reserves were depleted and during reperfusion injury. Furthermore, lactate may enhance antioxidant levels, slowing oxidative damage in nerve and muscle cells. This was in line with some medical studies suggesting that lactate played a pivotal role in metabolic regulation within the body [6,24].
In summary, our study's findings indicated a negative correlation between lactate levels and the occurrence of ICU-AW in the early stages of septic shock. We surmised that a slight increase in lactate levels might protect against the early development of ICU-AW in septic shock patients. Thus, lactate should not be simplistically regarded as a metabolic waste product; it may also have a potential protective role, providing new insights for future research and clinical applications.
Declarations
Declaration of interests: The authors have no conflict of interest to declare.
Funding: Guizhou Province High-level Innovative Talents Training Program (Qiancheng Talent [2022]201701); Qiandongnan Prefecture Science and Technology Support Program (Qiandongnan Kehe Support [2021]12).
References
- Taylor C. Intensive care unit acquired weakness [J]. Anaesthesia & Intensive Care Medicine. 2021; 22: 81-84.
- Vanhorebeek I, Latronico N, Van den Berghe G. ICU-acquired weakness [J]. Intensive Care Med. 2020; 46: 637-653.
- Kelmenson DA, Held N, Allen RR, et al. Outcomes of ICU patients with a discharge diagnosis of critical illness polyneuromyopathy: a propensity-matched analysis [J]. Crit Care Med. 2017; 45: 2055-2060.
- Kennedy L, Glesaaen ER, Palibrk V, et al. Lactate receptor HCAR1 regulates neurogenesis and microglia activation after neonatal hypoxia-ischemia [J]. Elife. 2022; 11: e76451.
- Annoni F, Peluso L, Gouvêa Bogossian E, et al. Brain protection after anoxic brain injury: Is lactate supplementation helpful? [J]. Cells. 2021; 10: 1714.
- Brooks GA, Arevalo JA, Osmond AD, et al. Lactate in contemporary biology: A phoenix risen [J]. J Physiol. 2022; 600: 1229-1251.
- Hall MM, Rajasekaran S, Thomsen TW, et al. Lactate: friend or foe [J]. PMR. 2016; 8: S8-S15.
- Nielsen OB, de Paoli F, Overgaard K. Protective effects of lactic acid on force production in rat skeletal muscle [J]. J Physiol. 2001; 536: 161-166.
- Bandschapp O, Soule CL, Iaizzo PA. Lactic acid restores skeletal muscle force in an in vitro fatigue model: are voltage-gated chloride channels involved? [J]. Am J Physiol Cell Physiol. 2012; 302: 1019-25.
- Chiu C, Legrand M. Epidemiology of sepsis and septic shock [J]. Curr Opin Anaesthesiol. 2021; 34: 71-76.
- Bakker J, Postelnicu R, Mukherjee V. Lactate: Where are we now? [J]. Crit Care Clin. 2020; 36: 115-124.
- Mok G, Hendin A, Reardon P, et al. Macrocirculatory and microcirculatory endpoints in sepsis resuscitation [J]. J Intensive Care Med. 2021; 36: 1385-1391.
- Hernández G, Ospina-Tascón GA, Damiani LP, et al. Effect of a resuscitation strategy targeting peripheral perfusion status vs serum lactate levels on 28-Day mortality among patients with septic shock: the ANDROMEDA-SHOCK randomized clinical trial [J]. JAMA. 2019; 321: 654-664.
- Yang WS, Kang HD, Jung SK, et al. A mortality analysis of septic shock, vasoplegic shock and cryptic shock classified by the third international consensus definitions (Sepsis-3) [J]. Clin Respir J. 2020; 14: 857-863.
- Ma H, Liu H, Wu C, et al. Diagnostic value of serum heparin binding protein, blood lactic acid combined with hs-CRP in sepsis and its relationship with prognosis [J]. Evid Based Complement Alternat Med. 2021; 2021: 5023733.
- Li XL, Yang YY, Zhang B, et al. Lactate metabolism in human health and disease [J]. Signal Transduct Target Ther. 2022; 7: 305.
- Lee S, Choi Y, Jeong E, et al. Physiological significance of elevated levels of lactate by exercise training in the brain and body [J]. J Biosci Bioeng. 2023; 135: 167-175.
- Brooks GA, Osmond AD, Arevalo JA, et al. Lactate as a myokine and exerkine: Drivers and signals of physiology and metabolism. J Appl Physiol (1985) [J]. 2023; 134: 529-548.
- Jourdain P, Allaman I, Rothenfusser K, et al. L-lactate protects neurons against excitotoxicity: Implication of an ATP-mediated signaling cascade [J]. Sci Rep. 2016; 6: 21250.
- Lauritzen KH, Morland C, Puchades M, et al. Lactate receptor sites link neurotransmission, neurovascular coupling, and brain energy metabolism [J]. Cereb Cortex. 2014; 24: 2784-95.
- Brooks GA, Osmond AD, Arevalo JA, et al. Lactate as a major myokine and exerkine [J]. Nat Rev Endocrinol. 2022; 18: 712.
- Oishi Y, Tsukamoto H, Yokokawa T, et al. Mixed lactate and caffeine compound increases satellite cell activity and anabolic signals for muscle hypertrophy [J]. J Appl Physiol (1985). 2015; 118: 742-9.
- Brooks GA, Curl CC, Leija RG, et al. Tracing the lactate shuttle to the mitochondrial reticulum [J]. Exp Mol Med. 2022; 54: 1332-1347.
- Brooks GA. Lactate as a fulcrum of metabolism [J]. Redox Biol. 2020; 35: 101454.