
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Boerhaave syndrome: A rare cause of sudden chest pain
Bruno Vieira*; Nádia Tenreiro; André Marçal; Gonçalo Guidi; Daniela Martins; João Pinto-de-Sousa
General Surgery Department, Hospital Center of Trás-Os-Montes and Alto Douro (CHTMAD), Clinical Academic Centre of Trás-os-Montes and Alto Douro (CACTMAD), Portugal.
*Corresponding Author : Bruno Vieira
General Surgery Department, Hospital Center of Trás-Os-Montes and Alto Douro (CHTMAD), Clinical Academic Centre of Trás-os-Montes and Alto Douro (CACTMAD), Av. Noruega, 5000-508, Vila Real, Portugal.
Tel: +351916596019;
Email: bruno.baiaovieirao@hotmail.com
bmbvieira@chtmad.min-saude.pt
Received : Dec 12, 2023
Accepted : Jan 03, 2024
Published : Jan 10, 2024
Archived : www.jcimcr.org
Copyright : © Vieira B (2024).
Keywords: Esophageal perforation; Rupture; Spontaneous; Hydropneumothorax pneumomediastinum; Esophageal exclusion.
Citation: Vieira B, Tenreiro N, Marçal A, Guidi G, Martins D, et al. Boerhaave syndrome: A rare cause of sudden chest pain. J Clin Images Med Case Rep. 2024; 5(1): 2789.
Description
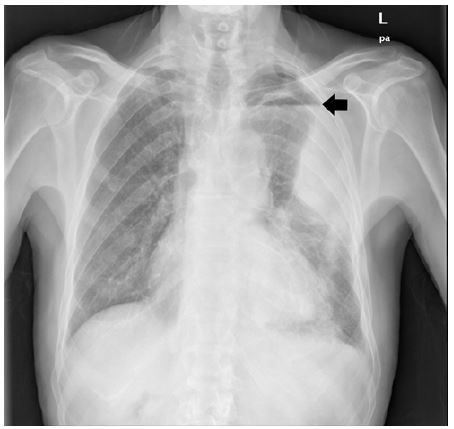
A 81-year-old man with previous history of arterial hypertension presented to the emergency department with sudden left chest pain and dyspnea, after having two episodes of non-bloody vomiting. He was hypotensive, tachycardic, with absent breath sounds on the left. Chest radiograph revealed left hydropneumothorax (Figure 1) and laboratory results showed hyperlactacidemia without other organ dysfunctions. CT scan confirmed hydropneumothorax, with associated pneumomediastinum and left lung consolidation (Figure 2), compatible with Booerhave´s syndrome. An anterior thoracic drain was placed. He was started on fluids, broad-spectrum antibiotics, and surgical consultation was obtained. Esophageal exclusion, feeding gastrostomy and left lateral thoracostomy were performed. Postoperatively, the patient was admitted to an intensive care unit. Unfortunately, the patient died on the post-operative day 8 due to respiratory infection. This case highlights the importance of considering esophageal perforation in the differential diagnosis of chest pain. Quick recognition of this condition is essential for appropriate management.

Declarations
Conflict of interest: None of the other authors has any conflict of interest to declare concerning this paper.
Funding: None.
References
- Díaz-Antonio T, Mirón Fernández I, Rodríguez Molina A. Perforación esofágica no iatrogénica (síndrome de Boerhaave). Cir Esp. 2021; 99: 308.
- Lieu MT, Layoun ME, Dai D, Soo Hoo GW, Betancourt J. Tension hydropneumothorax as the initial presentation of Boerhaave syndrome. Respir Med Case Rep. 2018; 25: 100-103.
- Wang J, Wang D, Chen J. Diagnostic challenge and surgical management of Boerhaave’s syndrome: a case series. J Med Case Reports. 2021; 15: 553.