
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Osteonecrosis of the lunate bone
Fadwa Jaheddine*
Department of Medical Imaging, Mohammed V University, 10100, Faculty of Medicine and Pharmacy, Rabat, Morocco.
*Corresponding Author : Fadwa Jaheddine
Microbial Biotechnology Department, National Research Centre, Cairo, EgyptDepartment of Medical Imaging, Mohammed V University, 10100, Faculty of Medicine and Pharmacy, Rabat, Morocco.
Email: fadwa.jhd@gmail.com
Received : Dec 06, 2023
Accepted : Jan 04, 2024
Published : Jan 11, 2024
Archived : www.jcimcr.org
Copyright : © Jaheddine F (2024).
Summary
ChordomaOsteonecrosis of the lunate bone or lunatomalacia, it is also known as Kienbok disease. The mechanisms by which this disorder develops are not fully understood, compromise of the bone vasculature is the most commonly proposed cause. MRI is useful in diagnosis and staging and should be considered after conventional radiography, for patients with suspected Kienböck disease.
Keywords: Osteonecrosis of the Lunate; Kienböck disease; Lunatomalacia; Wrist; MRI.
Citation: Jaheddine F. Osteonecrosis of the lunate bone. J Clin Images Med Case Rep. 2024; 5(1): 2792.
Case report
We report the case of a 31-year-old man patient who presented with dorsally located central wrist pain and tenderness around the lunate and limited motion.
The patient did not report any history of trauma.
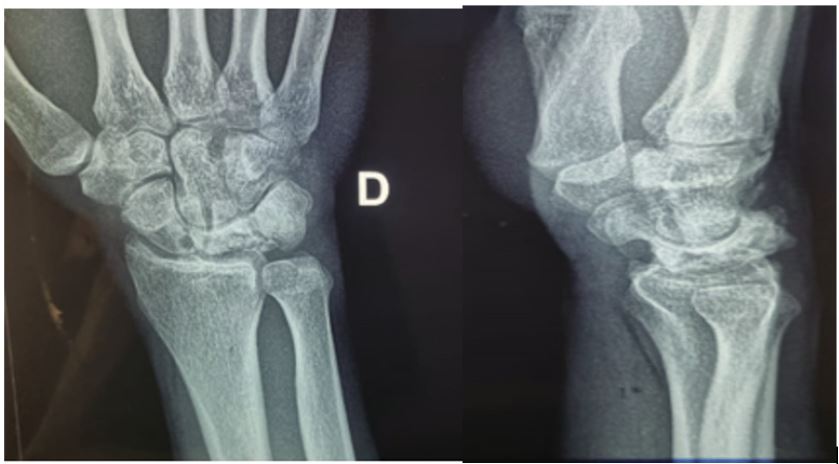
Plain radiograph showed sclerosis and flattening of the lunate (Figure 1).
MRI of the wrist was requested for diagnostic confirmation, which revealed collapse of the lunate with marrow signal changes (Figure 2).
Commentry
Kienböck’s disease is a rare condition, first described in 1910 by an austrian radiologist “Robert Kienböck”, characterized by aspetic osteonecrosis of the lunate. It is also known as lunatomalacia and aseptic or ischemic necrosis of the lunate [2].
The age range affected by this pathology is the young subject between 20 and 40 with a male predominance [2], it most often affects the dominant wrist, however bilateral involvement is possible, the clinic is non-specific hence the delayed diagnosis, the symptoms most frequently observed are pain and sensitivity of the central part of the wrist, limitation of movement with sometimes a carpal tunnel syndrome [3].
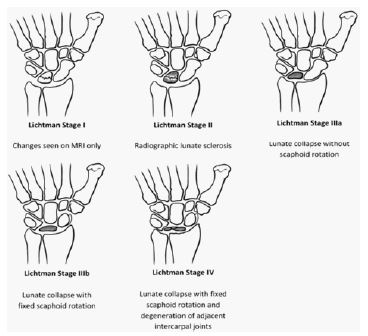
Imaging plays a vital role in the positive diagnosis and progression of the disease. Conventional radiography is often performed as the first line of defence and can reveal sclerosis and loss of height of the lunate bone, as well as signs of osteoarthritis; the Lichtman classification is more widely used in current practice, and is of therapeutic interest, allowing the disease to be staged into four progressive stages (Figure 3). Nevertheless, in early forms, standard radiography is often normal, hence the interest of magnetic resonance imaging.
MRI is the key examination, and is useful for differential positive diagnosis, evolution and post-treatment monitoring. MRI is also essential for diagnosing stage I Kienböck disease, defined by clinical symptoms of the wrist with normal radiographic findings. MRI diagnostic criteria are based on the collapse of the lunate bone and the change in bone marrow signal, most often manifested by low signal on T1 and heterogeneous high signal on T2 [3]. In addition, MRI is useful for longitudinal evaluation of the post-operative response to direct and indirect revascularization procedures. Contrast-enhanced MRI is important for determining the degree of tissue necrosis and the most appropriate treatment for stages II and IIIA disease. However, contrast injection is not necessary in stages I, IIIB, IIIC or IV, as the degree of necrosis does not affect treatment in these stages.

A. Coronal T1-weighted MR image shows hypointensity of lunate bone. B. Coronal T2-weighted fat-suppressed MR image shows mild increase on signal intensity in lunate bone. C. Sagittal fat-suppressed T2-weighted MR image shows collapse with mild increase on signal intensity in lunate bone. D. Coronal fat-suppressed T1-weighted MR image shows partial enhancement of lunate.
Conclusion
Kienböck disease is a condition that has been described for at least a century, with no obvious cause. Imaging is essential for positive, differential, evolutionary and surveillance diagnosis, hence the need for radiologists to be familiar with this condition and to disseminate its diagnostic criteria.
The treatment of Kienböck disease is still not consensual and numerous techniques are used to bring indolence, mobility and strength to patients.
References
- M Rahem, K Amimoussa, MK Larbaoui. Hand surgery and rehabilitation. 2018.
- J Arnaiz, T Piedra, L Cerezal, J Ward. American Journal of radiology. 2014.
- DW Stoller. Magnetic resonance imaging in orthopaedics and sports medicine, 3rd ed. Baltimore, MD: Lippincott Williams & Wilkins. 2007.
- Stuckey SL, Kalff V, Hoy G. Bone scan findings in Kienböck’s disease: A case report with atypical findings and literature review. Clin Nucl Med. 1997.
- Lichtman DM, Mack GR, MacDonald RI, Gunther SF, Wilson JN. Kienbock’s disease: The role of silicone replacement arthroplasty. J Bone Jt Surg Am. 1977; 59: 899-908.