
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Langerhans cell histiocytosis: Central nervous system findings
Belkouchi Lina*; Selma Khouchoua; Siham El Haddad; Nazik Allali; Latifa Chat
Department of Radiology, Children Hospital of Rabat, Faculty of medicine and pharmacy of Rabat, Morocco.
*Corresponding Author : Belkouchi Lina
Department of Radiology, Children Hospital of Rabat, Faculty of Medicine and Pharmacy of Rabat, Morocco.
Tel: +212-659-14 27-87;
Email: belkouchilina@gmail.com
Received : Dec 17, 2023
Accepted : Jan 05, 2024
Published : Jan 12, 2024
Archived : www.jcimcr.org
Copyright : © Lina B (2024).
Citation: Lina B, Khouchoua S, El Haddad S, Allali N, Chat L. Langerhans cell histiocytosis: Central nervous system findings. J Clin Images Med Case Rep. 2024; 5(1): 2793.
Case description
A 4-year-old boy was admitted for polyuria and polydipsia syndrome for which the diagnosis of diabetes insipidus was retained after doing a hydrous restriction test with the Minirin test.
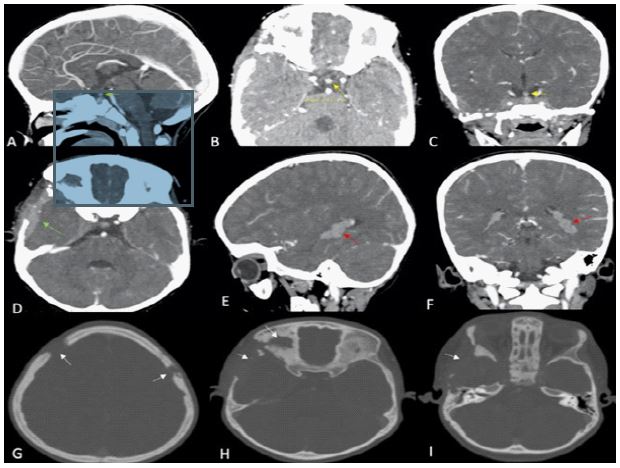
A brain CT scan performed revealed thickening of the pituitary stalk (4 mm) (Figure 1 yellow arrows A, B, C), thickening of the dura mater (Figure 1 green arrow, D), abnormal thickening of the left choroid plexus (Figure 1 red arrow F) and cranio-facial skull lesions (Figure 1 white arrows G, H, I).
Discussion
Langerhans cell histiocytosis is a rare multisystemic disease due to an anomaly in the monocyte macrophage system causing uncontrolled monoclonal proliferation of Langerhans cells. It is more common within children. It frequently affects bones and skin [1-4].
Central nervous system lesions only occur in about 5-10% of the cases.
They include:
1- Anomalies of the hypothalamic-pituitary-adrenal axis:
- Enhancement and thickening of the pituitary stalk >3 mm.
- MRI shows a loss of the physiological high signal intensity of the posterior pituitary on T1 weighted images without contrast.
2- Craniofacial and skull destructive lytic lesions, best seen on a CT scan, MRI shows iso/hyperintense lesions on T2 weighted images, enhancing on post-contrast.
3- Grey matter anomalies: Bilateral and symmetrical hyperintense signal in T1 and T2 weighted images of both the dentate nucleus and basal ganglia.
4- Masses and thickening of the dura mater, masses of the pineal gland, the choroid plexus, or the hypothalamus.
Diagnosis confirmation requires a histological examination of either extra or intra cranial lesions.
Treatment depends on whether the disease is single located of multisystemic.
There’s no standard treatment for central nervous system histiocytosis. It often involves: prednisolone/dexamethasone, low dose radiation therapy, chemotherapy, and/or surgical resection, however, it may not be always effective.
References
- Fleur Cohen Aubart, et al. Histiocytosis and the nervous system: From diagnosis to targeted therapies. Neuro-Oncology. 2021.
- Loïc Le Guennec et al. Neurohistiocytose langerhansienne. La presse médicale. 2016.
- Luciana Porto, et al. Central nervous system imaging in childhood Langerhans cell histiocytosis- a reference center analysis. Radiology and Oncology. 2015.
- Zachary C Gersey, et al. Intracranial Langerhans cell Histiocytosis: A review. Interdisciplinary Neurosurgery. 2020.