
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Arthroscopic resection of large synovial hemangioma in the posterior recess of the left knee via median and double posteromedial portals: A case report
Xin Mu1,2; Menghao Li2; Shicheng Jia2; Shengbo Lu2; Jiayou Chen2; Jianjing Lin2; Wei Li2*
1Department of Sports Medicine, Clinical College of Anhui Medical University, Peking University Shenzhen Hospital, Lianhua Road 1120, Futian District, Shenzhen 518036, Guangdong, People’s Republic of China.
2Department of Sports Medicine, Peking University Shenzhen Hospital, Lianhua Road 1120, Futian District, Shenzhen 518036, Guangdong, People’s Republic of China.
*Corresponding Author : Wei Li
Department of Sports Medicine, Peking University Shenzhen Hospital, Lianhua Road 1120, Futian District, Shenzhen 518036, Guangdong, People’s Republic of China.
Email: lwjnu2003@126.com
Received : Dec 14, 2023
Accepted : Jan 05, 2024
Published : Jan 12, 2024
Archived : www.jcimcr.org
Copyright : © Li W (2024).
Abstract
Synovial hemangioma is a rare benign tumor. This case report describes a 27-year-old woman who was admitted to the hospital with a 1-year history of pain in the popliteal fossa of the left knee and mobility limitation. According to the medical history and MRI examination, the patient was diagnosed as synovial hemangioma of the left knee joint, and finally underwent arthroscopic surgery. The location of the mass was in the posterior recess of the knee joint and its size was large, so it was difficult to respect the mass by traditional anteromedial and anterolateral portals. Therefore, we used arthroscopy to remove the mass in the posterior recess of the knee through a double posteromedial portal completely. The resected mass was sent for pathological examination, which confirmed synovial hemangioma. MRI showed no recurrence at 8 months after operation.
Keywords: Synovial hemangioma; Arthroscopic surgery; Double posteromedial portal.
Citation: Mu X, Li M, Jia S, Lu S, Li W, et al. Arthroscopic resection of large synovial hemangioma in the posterior recess of the left knee via median and double posteromedial portals: A case report. J Clin Images Med Case Rep. 2024; 5(1): 2794.
Introduction
Synovial hemangioma is a rare benign tumor, which accounts for only 0.07% of all soft tissue tumors [1], mostly occurring in the synovial membrane of the knee, elbow and finger joints of children and adolescents. Synovial hemangioma of the knee joint is most common in the anterior suprapatellar and patellofemoral space, and rarely occurs in the posterior recess of the left knee. The symptoms and signs of synovial hemangioma of the knee in most patients are non-specific, which is one of the reasons why the disease is easily misdiagnosed. The clinical manifestations are usually persistent pain, swelling and hemarthrosis [2]. X-rays and MRI are usually used for diagnosis. Open synovectomy is the most commonly used treatment method, while arthroscopic synovectomy is relatively less. However, there is still no conclusion about which of the two surgical methods is more advantageous. For synovial hemangiomas of the knee joint with a wide range of lesions, large volume, or involving the surrounding important tissues and organs, doctors are often more inclined to take open surgery [2,3]. In this case, although MRI showed that the tumor volume was large, we tried arthroscopic resection of the large mass through a double posteromedial portal, and obtained good surgical results.
Case presentation
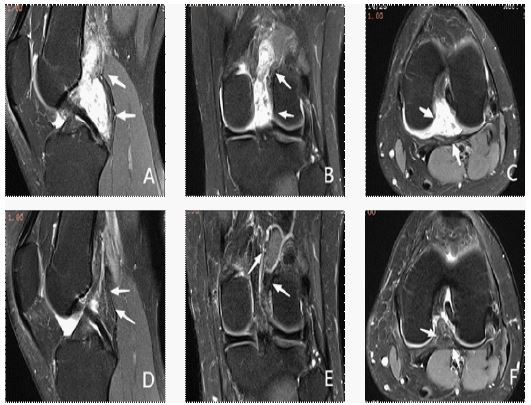
A 27-year-old female patient was admitted to the hospital due to pain in the popliteal fossa of the left knee with limitation of movement for 1 year and aggravation for 1 month. On physical examination, the left popliteal fossa was tender and no mass was palpable. When squatting, she felt pain and swollen in the popliteal fossa of the left knee. Her knee Range of Motion (ROM) was 0°to 120°. The Lasholm score was 85, the pain score VAS was 4. MRI showed a mass in the left knee capsule and popliteal fossa, which was considered to be synovial origin (Figure 1A-C). Preoperative diagnosis was synovial hemangioma of the left knee.
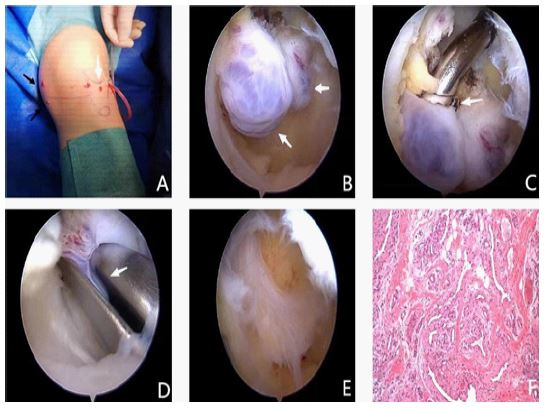
We obtained access to the posterior knee capsule through a double posteromedial portal (Figure 2A) and observed the posterior mass, which is multiple, pedunculated, grape-shaped, purple-red (Figure 2B). Then the mass was separated with radiofrequency ablation (Figure 2C) and removed with nucleus pulpous forceps (Figure 2D-E).
Using arthroscopy, we entered the knee joint through anteromedial and anterolateral portals, then entered the posterior recess through the gap between the anterior and posterior cruciate ligaments, and extended the knee joint slightly. We found a grape-shaped, purple mass on the upper part of the anterior and posterior cruciate ligaments of the knee joint, which was the poster superior portion of the mass. Then we flexed the knee slightly and removed the mass with a nucleus pulpous forceps through a longitudinal median portal. The resected tumor was sent for pathological examination. Intraoperative blood loss was 10 ml, and a drainage tube was placed within 24 hours after surgery. Pathological examination showed hemangioma (Figure 2F). After operation, the patient was instructed to strengthen functional exercise. At the 8th month follow-up, the Lasholm score was 95, the VAS score was 0, the left knee ROM was 0°to 130°. The symptoms and function were significantly improved. Re-examination of MRI showed that the original lesion completely disappeared without recurrence (Figure 1D-F).
Discussion
Recurrent swelling and intermittent pain of the knee are the typical symptoms [4]. Due to the lack of specific clinical manifestations and low incidence of synovial hemangioma of the knee, it is easy to be misdiagnosed or missed in clinical practice. When synovial hemangioma of the knee invades the ligaments, menisci, and even the femur [5], it can cause degenerative changes of joints in the long term, finally leading to the occurrence of osteoarthritis [6]. MRI plays an important role in the diagnosis [7]. The enhanced T2WI showed heterogeneous enhancement [8], which could be differentiated from cystic synovial hyperplasia, intra-articular hematoma and joint effusion [9]. However, it is important to emphasize that large venous hemangiomas can be hyperintensity on T1WI and areas of hyperintensity on T2WI or fat-suppressed T2WI, because of slow flow [10]. The main differential diagnosis of synovial hemangioma of the joint is villonodular synovitis, synovial sarcoma, and hemophilic arthropathy. In particular, nodular synovitis with pigmented features and synovial hemangioma of the knee joint are difficult to be distinguished clinically [7,9]. It is that the former shows low signal changes on T2-WI, and the latter shows high signal changes on T2-WI, which can be one of the bases to identify the two lesions, although the interference of intra-articular hemorrhage or steatosis cannot be ruled out [11]. In this case, the MRI appearance of synovial hemangioma was consistent with the typical imaging findings described above. Combining with the medical history of persistent and chronic pain in the popliteal fossa of knee, the diagnosis of synovial hemangioma of the knee should be considered.
Synovial hemangioma originates from the subsynovial mesenchymal cells. According to the histological characteristics, it can be divided into venous type, capillary type, arteriovenous type and cavernous type [3,12]. Compared with histological classification, the classification based on anatomical location is more significant in helping to choose the surgical method and judge the surgical effect. Keiichi et al. proposed another classification based on anatomical location including anterior patellofemoral joint type, posterior popliteal type, and diffuse hyperplasia type [3]. They suggested that resection of the patellofemoral joint type is relatively straightforward, because the tumor forms a simple nodule. In contrast, diffuse hyperplasia type and posterior popliteal type of synovial hemangiomas usually invade the posterior cruciate ligament and posterior part of the meniscus, which makes them difficult to completely remove [3]. In this case, although the characteristics of the synovial hemangioma were consistent with the popliteal posterior type and larger in size, no ligament and meniscus involvement was found on MRI, and the tumor was connected with normal tissue with a clear boundary and complete capsule, which were conducive to the complete resection of the tumor.
In terms of surgical methods, due to the large volume and irregular shape of synovial hemangioma, longitudinal and S-shaped incision are usually selected in traditional open surgery, but there are limitations such as causing large surgical trauma and scar. In contrast, arthroscopy can provide a clearer surgical field of view and avoid unnecessary injury. In addition, irrigation of the joint cavity can be performed more thoroughly under arthroscopy, and good hemostasis can be achieved using radiofrequency ablation. Previously, arthroscopic resection of synovial hemangiomas has been reported in a number of cases [8,13,14], with follow-up ranging from 6 months to 2 years and no recurrence. In this case, according to the results of imaging examination, we judged that the mass could be removed through arthroscopy. Specially, the tumor located in the posterior knee capsule. The selection and modification of the surgical portal are particularly important, so we optimized the surgical portal. We chose double posteromedial portal, through which we were able to observe the tumor throughout the operation, for the resection of the massive tumor in the posterior part of the anterior and posterior cruciate ligaments. Straighting the knee joint slightly, we successfully resected the upper mass behind the anterior cruciate ligament through the gap between the anterior and posterior cruciate ligaments. The postoperative symptoms of most patients with synovial hemangioma of the knee joint can be significantly improved. In this case, the patient avoided strenuous activities of the knee joint for 1 month after surgery, and the pain of the knee almost disappeared at the follow-up of 8 months after surgery. Postoperative MRI further confirmed the complete resection of the tumor.
Conclusion
Synovial hemangioma is a rare benign tumor, which mostly occurs in the knee joint. The clinical manifestations are usually persistent pain, swelling and hemarthrosis. MRI plays an important role in diagnosing synovial hemangioma of knee joint and guiding surgical treatment. For the surgical treatment of this case, we selected arthroscopic resection of the mass, and optimized the surgical portal. The massive mass was completely resected, which proved the advantages of double posteromedial portal in the resection of mass in the posterior recess of the knee.
Declarations
Author contributions: All authors have accepted responsibility for the entire content of this manuscript and approved its submission.
Competing interests: Authors state no conflict of interest.
Informed consent: Informed consent was obtained from all individuals included in this study.
Ethical approval: Research involving human subjects complied with all relevant national regulations, institutional policies and is in accordance with the tenets of the Helsinki Declaration (as revised in 2013), and has been approved by the authors’ Institutional Review Board (Peking University Shenzhen Hospital).
Funding disclosures/conflicts of interest: The authors declare no conflicts of interest and do not have any financial disclosures.
References
- Price NJ, Cundy PJ. Synovial Hemangioma of the Knee J Pediatr Orthoped. 1997; 17: 74-7.
- Hernández Hermoso JA, Moranas Barrero J, García-Oltra E, Collado-Saenz F, López Marne S. Location, Clinical Presentation, Diagnostic Algorithm and Open vs. Arthroscopic Surgery of Knee Synovial Haemangioma: A Report of Four Cases and a Literature Review. Front Surg. 2021; 7: 792380.
- Muramatsu K, Iwanaga R, Sakai T. Synovial hemangioma of the knee joint in pediatrics: Our case series and review of literature. Eur J Orthop Surg TR. 2019; 29: 1291-6.
- Wirth T, Rauch G, Rüschoff J, Griss P. Synovial haemangioma of the knee joint. INT Orthop. 1992; 16: 130-2.
- Silit E, Mutlu H, Pekkafali Z, Kizilkaya E, Basekim C. Synovial hemangioma of the knee invading the femur. Skeletal Radiol. 2002; 31: 612-4.
- Ramseier LE, Exner GU. Arthropathy of the Knee Joint Caused by Synovial Hemangioma: J Pediatr Orthoped. 2004; 83-6.
- Guler I, Nayman A, Koplay M, Paksoy Y. Synovial Hemangioma of the Knee Joint: Magnetic Resonance Imaging Findings. Pol J Radiol. 2015; 80: 450-2.
- Sasho T, Nakagawa K, Matsuki K, Hoshi H, Saito M, et al. Two cases of synovial haemangioma of the knee joint: Gd-enhanced image features on MRI and arthroscopic excision. The Knee. 2021; 18: 509-11.
- Larbi A, Viala P, Cyteval C, Snene F, Greffier J, et al. Imaging of tumors and tumor-like lesions of the knee. Diagn. Interventional Imaging. 2016; 97: 767-77.
- Hospach T, Langendörfer M, Kalle TV, Tewald F, Wirth T, et al. Mimicry of lyme arthritis by synovial hemangioma. Rheumatol Int. 2011; 31: 1639-43.
- Sonobe T, Hakozaki M, Kaneuchi Y, Yamada H, Hasegawa O, et al. Radiological and pathological characteristics of synovial hemangioma of the knee. Expther Med. 2022; 25: 23.
- Devaney K, Vinh TN, Sweet DE. Synovial hemangioma: A report of 20 cases with differential diagnostic considerations. Hum. Pathol. 1993; 24: 737-45.
- Meislin RJ, Parisien JS. Arthroscopic excision of synovial hemangioma of the knee. Arthroscopy: The Journal of Arthroscopic and Related Surgery. 1990; 6: 64-7.
- Wu Y, Qi Y, Li X, Luo W. Arthroscopic treatment of synovial hemangioma of the knee: A case report. Asian J Sugr. 2023; 46: 3825-6.