
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Chilaiditi syndrome: A simple chest x-ray image makes the diagnosis
Anwar Rahali*; Mohammed Rebbani; Noureddine Njoumi; Yasser El Brahmi; Mohammed Elfahssi; Abderrahman Elhjouji; Aziz Zentar; Abdelmounaim Ait Ali
Department of Visceral Surgery, Faculty of Medicine and Pharmacy, Mohammed V Military Teaching Hospital, Mohamed V University, Rabat, Morocco.
*Corresponding Author : Anwar Rahali
Senior Resident, General Surgery, Department of Visceral Surgery II, Mohammed V Military Teaching Hospital, Mohamed V University, Faculty of Medicine and Pharmacy, Rabat, Morocco.
Email: rahali.anwar87@gmail.com
Received : Dec 19, 2023
Accepted : Jan 10, 2024
Published : Jan 17, 2024
Archived : www.jcimcr.org
Copyright : © Rahali A (2024).
Keywords: Chilaiditi syndrome; Chest x-ray image; Diagnosis; Bowel obstruction.
Citation: Rahali A, Rebbani M, Njoumi N, El Brahmi Y, Elfahssi M, et al. Chilaiditi syndrome: A simple chest x-ray image makes the diagnosis. J Clin Images Med Case Rep. 2024; 5(1): 2801.
Description
Chilaiditi syndrome is the colonic interposition to the liver reaching the under-surface of diaphragm with associated abdominal pain; it is one of the causes of pseudopneumoperitoneum. This clinical manifestation distinguishes chilaiditi syndrome from asymptomatic colonic interposition, which is termed as chilaiditi sign [1,2].
A chest x-ray image confirms the diagnosis by showing gas between the liver and diaphragm. CT-scan can be performed to define whether there is pneumoperitoneum if abdominal visceral perforation is suspected [1,3].
Symptomatic patients with chilaiditi syndrome are usually treated conservatively with analgesia. Patients with evidence of bowel ischemia may be offered surgical treatment [1,4].
We report a case of a 43-year-old-man, with pathological history of intermittent and diffuse abdominal pain without intestinal transit disorder. The patient developed acute onset of epigastric pain and postprandial vomiting. He presented to the emergency department 12 hours after the beginning of symptoms. A physical examination revealed haemodynamically stable patient and abdominal distension.
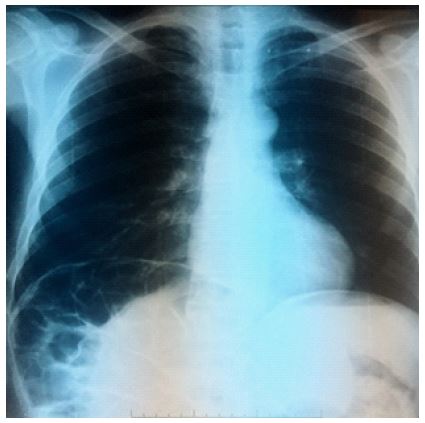
Routine laboratory tests were without anomalies. A chest x-ray image showed colonic interposition between the liver and diaphragm; the findings were suggestive of chilaiditi sign (Figure 1).
The symptoms gradually disappeared; the patient was discharged on day 3 after receiving conservative treatment and complete oral feeding resumption. He was reviewed in consultation four weeks later, the clinical examination was unremarkable.
References
- Jones J, El-Feky M, Skalina T, et al. Chilaiditi syndrome. Radiopaedia.org. 2021.
- Bin Waqar SH, Mohiuddin O, Khan AA, Ehtesham M. Gut Entrapped in the Thorax: A Rare Presentation of Abdominal Pain in Chilaiditi Syndrome. Cureus. 2019; 11: e5180.
- Asanad S, Tewoldemedhin B, Singh S, Sood A, Michael MB. Thoracic Gut Entrapment Presenting As Intractable Hypoxia: A Case Report of Chilaiditi Syndrome. Cureus. 2022; 14: e25963.
- Guirguis MM, Horawski J, Gibbs SL. Chilaiditi Sign in a Patient With Acute Coronary Syndrome: A Case Report. Cureus. 2023; 15: e36237.