
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Systemic artery to pulmonary artery fistula
Atif Siddiqui*
Department of Medicine, Division of Pulmonary and Critical Care Medicine, Houston Methodist Hospital, Houston, Texas, USA.
*Corresponding Author : Atif Siddiqui
Houston Methodist Hospital 6550 Fannin St. Suite 2321 Houston, Texas 77030, USA.
Email: asiddiqui@houstonmethodist.org
Received : Dec 19, 2023
Accepted : Jan 10, 2024
Published : Jan 17, 2024
Archived : www.jcimcr.org
Copyright : © Siddiqui A (2024).
Keywords: Shortness of breath; Pulmonary artery fistula; Intervention.
Citation: Siddiqui A. Systemic artery to pulmonary artery fistula. J Clin Images Med Case Rep. 2024; 5(1): 2802.
Description
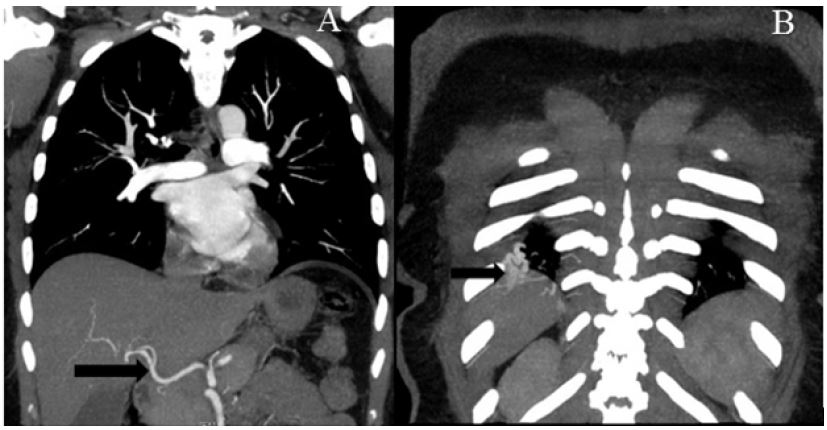
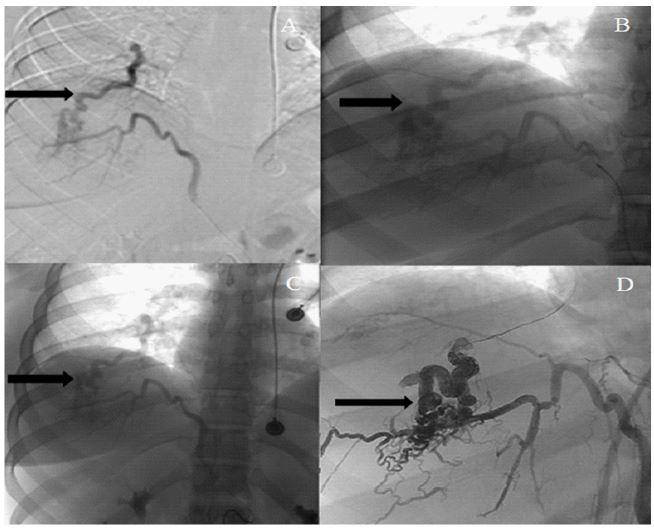
A 33-year-old female presented with four years of shortness of breath. She denied sputum production, fever, chills, chest pain or hemoptysis. She was diagnosed with pulmonary embolism four years prior, treated with anticoagulation for six months. Physical examination was remarkable for sinus tachycardia. Echocardiogram along with pulmonary function tests and diffusion coefficient were normal. Chest Computed Tomography (CT) angiogram showed Inferior Phrenic Artery (IPA) to Pulmonary Artery (PA) communication. A dilated right IPA was seen supplying the vascular malformation in the Right Lower Lobe (RLL), measuring approximately 1.9x1.1 cm (Figure 1). Phrenic arteriogram showed a complex vascular malformation supplied by the right IPA branches and draining into a dilated branch of the RLL PA (Figure 2).
She underwent successful embolization of the IPA-PA fistula using arterial to arterial approach with onyx embolization material and coils.
Systemic-PA fistulas, an extremely rare, cause of filling defects in pulmonary arteries, should be suspected with atypical presentations and imaging findings. Diagnosis is confirmed by delayed contrast-enhanced CT or conventional pulmonary angiography. Trans catheter embolization is a feasible therapeutic option. No definitive treatment guidelines are established, but some recommend treatment to avoid complications including hemoptysis, pulmonary hypertension, and congestive heart failure [1-3].
Funding: None.
Conflicts of interest: None.
References
- Yakushiji E, Ota S, Komatsu T, Ayaori M, Ikewaki K. Massive Hemoptysis due to Right Inferior Phrenic Artery-to-Right Pulmonary Artery Fistula in the Right Middle Lobe of the Lung. Intern Med. 2017; 56: 687-689.
- Lee JK, Park JH, Kim J, Kim SJ, Lee AR, et al. Embolization of Multiple Systemic Artery to Pulmonary Artery Fistula with Recurrent Hemoptysis. Tuberc Respir Dis (Seoul). 2013; 75: 120-4.
- Geyik S, Yavuz K, Keller FS. Unusual systemic artery to pul¬monary artery malformation without evidence of systemic disease, trauma or surgery. Cardiovasc Intervent Radiol 2006; 29: 897-901.