
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Infantile scapulothoracic dissociation
Arash Maleki1*; Hossien Moaddabi2; Amir Bisadi3; Ghazal Valinejad4
1Assistant Professor, Akhtar Hospital, SBMU, Tehran, Iran.
2Orthopaedic Surgeon, Akhtar hospital, SBMU, Tehran, Iran.
3Assistant Professor, Akhtar Hospital, SBMU, Tehran, Iran.
3General Practitioner, Akhtar hospital, SBMU, Tehran, Iran.
*Corresponding Author : Arash Maleki
Clinical Research & Development Unit, Akhtar Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Email: arashmal@yahoo.com
Received : Dec 27, 2023
Accepted : Jan 11, 2024
Published : Jan 18, 2024
Archived : www.jcimcr.org
Copyright : © Maleki A (2024).
Abstract
Scapulothoracic dissociation is rare but a limb-threating injury that usually occurs after high energy trauma. Our case was 2 year olds after low energy trauma with axillary mas and restricted movement of the right shoulder and radiographic finding showed that the scapula was displaced laterally. He was immobilized with shoulder spica for 4 weeks. Scapulothoracic dissociation in children can occur after low energy trauma and this injury would have a good prognosis with casting, if he had no neuro-vascular injuries.
Keywords: Scapulothoracic dissociation; Casting; Vascular injury.
Citation: Maleki A, Moaddabi H, Bisadi A, Valinejad G. Infantile scapulothoracic dissociation. J Clin Images Med Case Rep. 2024; 5(1): 2806.
Introduction
Scapulothoracic dissociation is a rare injury that described the separation of the scapula and upper extremity from the thorax. It is a limb-threatening injury that usually occurs after high energy trauma [1]. Sometimes it is concomitant with neurovascular injury and a poor prognosis is induced [2]. Scapulothoracic dissociation in children hasn’t been reported so, we haven’t any guide for its treatment.
Case presentation
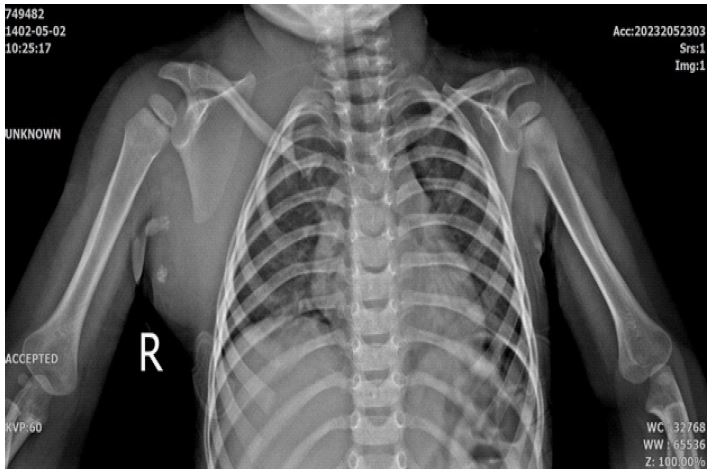
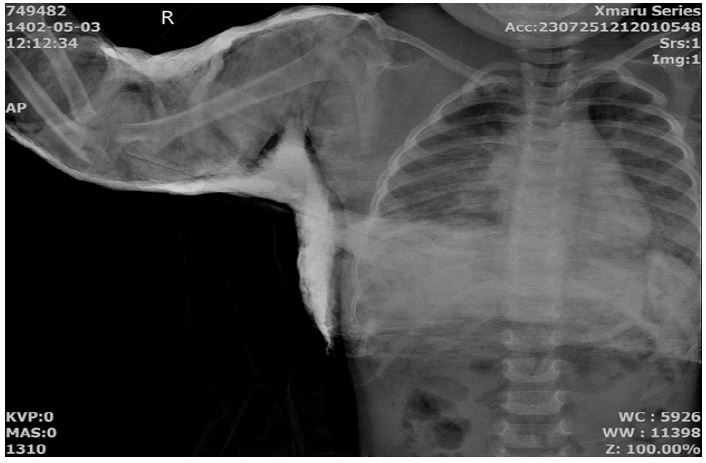
Our case was a 24 month old boy who was referred to our hospital for Scapulothoracic dissociation after upper extremity manipulation after one week. He was irritable and he didn’t move his shoulder, but active motion in the distal extremity (elbow, wrist and fingers) was normal and he resisted to any passive movement of the right shoulder. A cleft was seen on superolateral of right nipple on chest wall without any skin finding such as abrasion or laceration but deep muscular defect was detected on touching anterior of chest wall. A firm pulseless mass was detected in right axillary fold. The radial and ulnar arteries were symmetric in both upper extremities. Normal neurologic findings with Nerve Conduction Velocity (NCV) were approved. Radiographs of the patient showed that the shoulder, scapula and clavicle were displaced laterally without a clear fracture that detected dislocation and displacement in the sternoclavicular joint and the scapula-ribs junctions (Figure 1) some calcification were detected on axillary fold that lymph node was reported on sonography. Infant was immobilized in shoulder spica casting after trying to translated scapula and upper extremity medially for 4 weeks (Figure2). After 4 weeks, the cast was removed and his shoulder and upper extremity actively moved so that neurovascular examination was normal. The displacement of the scapula decreased in the follow up radiography at 2 months (Figure 3) and 4 months (Figure 4) after casting. Axillary calcifications were remained on the last radiography.


Discussion
Motorcycle accidents are the most common cause of Scapulothoracic dissociation. Other causes are automobile accident, fall from height [3,4]. Scapulothoracic dissociation is a limb-threatening injury that occurs after high energy trauma and is associated with multiple injuries such as long bone fractures, although it is a rare injury. This injury may be associated with neurovascular injuries [2,5]. A massive traction injury is the usual cause leading to the articular disruption of the Scapulothoracic junction, the same as our case which can induce neurologic defect such as brachial plexus avulsion, subclavian or axillary artery injury, extensive muscular and osseous injuries [6]. Our case hadn’t major trauma and his skin was intact, diagnosis may be missed easily only careful attention on his chest radiography suggested lateral scapula displacement. Misdiagnosis may be higher in a poly-trauma situation and high suspicion is essential for diagnosis [6]. The scapulae normally articulate with the 2-7 ribs that this articulation lost in the Scapulothoracic dissociation. And dissociation will be suggested if the scapula displaced more than 1 cm laterally [6]. A screening tool for diagnosing Scapulothoracic dissociation is the Scapular Index described by Kelbel [7]. The normal value is 1.07 ± 0.04 [8] this index didn’t have any correlation with the final functional outcomes or predicted the vascular or brachial plexus injuries. Also, this index had low sensitivity and specificity because the main problem is difficult to get non-rotated view of scapula [6]. CT angiography plays an important role in assessing the vascular injury and determining revascularization procedures [6]. In our case, radial and ulnar arteries pulses were regular and we didn’t used CT angiography. MRI and electro-diagnostic studies are helpful in assessing the neurological status [6]. That our case had normal EMG-NCV findings. Management depends on many factors such as neurologic or vascular conditions and associated thoracic and abdominal injuries, because this is often the result of high energy trauma [9]. Careful observation is recommended for the non-ischemic limb but ischemic limbs may have poor prognosis and may progress to early amputation or death [1]. However, Scapulothoracic dissociation was rare and it hasn’t been reported in children. Low energy trauma can induce this injury in children and conservative treatment may be a good choice in intact neurovascular situation.
References
- Alharbi AA, Abbas AMN, Mousa WF. Scapulothoracic Dissociation without a Neurological Compromise: A Case Report. Egyptian Journal of Hospital Medicine. 2022; 88.
- Taufeeq A, McConnell JS. Scapulothoracic dissociation following blunt trauma. BMJ Case Reports. 2013.
- Ebraheim NA, Pearlstein SR, Savolaine ER, Gordon SL, Jackson WT, et al. Scapulothoracic dissociation (Closed avulsion of the scapula, subclavian artery, and brachial plexus): A newly recognized variant, a new classification, and a review of the literature and treatment options. J Orthop Trauma. 1987; 1.
- Oreck SL, Burgess A, Levine AM. Traumatic lateral displacement of the scapula: A radiographic sign of neurovascular disruption. Journal of Bone and Joint Surgery-Series A. 1984; 66.
- Choo AM, Schottel PC, Burgess AR. Scapulothoracic dissociation: Evaluation and management. Journal of the American Academy of Orthopaedic Surgeons. 2017: 25.
- Kumar V, Bhayana H, Salaria AK, Neradi D, Aggarwal S, et al. Scapulothoracic Dissociation: A Systematic Review, Current Concepts, and Meta-analysis of Case Reports. SN Comprehensive Clinical Medicine. 2020; 2: 2884-9.
- Zelle BA, Pape HC, Gerich TG, Garapati R, Ceylan B, et al. Functional Outcome Following Scapulothoracic Dissociation. Journal of Bone and Joint Surgery. 2004; 86.
- Kelbel JM, Jardon OM, Huurman WW. Scapulothoracic dissociation: A case report. Clin Orthop Relat Res. 1986; 209.
- Jbara M, Bajwa J, Hahn B. Scapulothoracic dissociation. Journal of Emergency Medicine. 2013; 44.