
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 5
Clinico-pathological characteristics of triple negative breast cancer: A retrospective study of 50 cases
Ihssan Elouarith1*; Yassine Bouhtoui2; Dounia Benaich1; Jaouad Kouach2; Mohamed Oukabli1
1Pathology Department, Military Hospital of Instruction Mohamed V, Rabat, Morocco.
2Department of Gynecology and Obstetrics, Military Hospital of Instruction Mohamed V, Rabat, Morocco.
*Corresponding Author : Ihssan Elouarith
Pathology Department, Military Hospital of Instruction Mohamed V Rabat, Faculty of Medicine and Pharmacy, Mohammed V University, 10100 Rabat, Morocco.
Email: i.elouarith@gmail.com
Received : Dec 26, 2023
Accepted : Jan 12, 2024
Published : Jan 19, 2024
Archived : www.jcimcr.org
Copyright : © Elouarith I (2024).
Abstract
Objective: Retrospective study aimed to investigate the anatomo-clinical features of triple negative breast carcinoma and compare them with data in the literature.
Method: An exhaustive retrospective study of 50 cases of triple-negative breast cancer diagnosed in the Pathology Department at the Mohammed V Military Training Hospital in RABAT, for five years and 08 months from January 2018 to August 2023.
Result: The incidence of Triple-Negative Breast Cancer (TNBC) was 11, 87% and the mean age of the patients was 48, 84 years. The most frequent reason for consultation was the discovery of breast nodules. The most frequent histological type was non-specific infiltrating carcinoma in 78% of cases. The Scarff-Bloom-Richardson histopronostic grade for our patients was SBR III in 75.60%. On immunohistochemistry, ER and PR were absent in 100% of our patients, HER2 was 0 in 64.51%, 1 in 16.12% and 2 in 19.35%. The Ki 67 proliferation index was >14% in 84.51% of cases.
Conclusion: The results of our study are consistent with the literature. Triple-Negative Breast Cancer (TNBC) is a clinically, morphologically, molecularly and prognostically heterogeneous subgroup of breast cancer, requiring multidisciplinary collaboration and the search for new targeted therapy to optimize its management.
Keywords: Clinic pathological; Characteristics; Triple negative breast cancer.
Citation: Elouarith I, Bouhtouri Y, Benaich D, Kouach J, Oukabli M. Clinico-pathological characteristics of triple negative breast cancer: A retrospective study of 50 cases. J Clin Images Med Case Rep. 2024; 5(1): 2807.
Introduction
Breast cancer is the most common cancer in women and the leading cause of death from cancer in women [1]. In Morocco, it is a public health problem, affecting young women with a steadily increasing incidence [2,3]. Advances in the analysis of transcriptomic expression profiles of invasive breast carcinomas have led to a better understanding and classification of breast carcinology, and effective adaptation of therapeutic approaches [4,5]. Triple-Negative Breast Cancer (TNBC) is a heterogeneous subgroup of breast tumors, with few therapeutic options, characterized by a lack of expression of Estrogen and Progesterone hormone Receptors (ER and PR) and an absence of HER2 overexpression and amplification. A recent classification based on TNBC gene expression data has individualized four specific subtypes: basal-like 1 and basal-like 2 (differing in immune response), mesenchymal, and luminal AR (Androgen Receptor). These subtypes have different survival rates and sensitivity to neoadjuvant chemotherapy [5]. Current research seeks to identify specific therapeutic targets based on genomic studies to improve the prognosis of this type of cancer. Our retrospective study aimed to investigate the anatomo-clinical features of TNBC and compare them with data in the literature.
Material and methods
Type of study: An exhaustive retrospective study of 50 cases of triple-negative breast cancer diagnosed in the Department of Anatomy and Pathological Cytology at the Mohammed V Military Training Hospital in RABAT, for five years and 08 months from January 2018 to August 2023.
Inclusion criteria
- Patients with histologically confirmed breast cancer during the study period.
- Absence of hormone receptor expression: RE - ; RP -.
- Absence of HER2 expression or amplification (her2 negative or low).
Exclusion criteria
- Patients who did not benefit from a complete histological analysis,
- Male gender.
- Incomplete clinical records.
Data collection relied on detailed operative charts for each patient.
Text and tables input using Word XP, and graphs using Excel XP.
Statistical analysis was accomplished using SPSS version 24 software.
Results
General characteristics: Over a period of five years and 08 months, from January 2018 to August 2023 inclusive, 50 women had triple-negative breast cancer among 421 women with breast cancer diagnosed at the pathology department of the Mohammed V Military Training Hospital in RABAT. I.e. A frequency of 11.87% of the total number of breast cancers. The mean age of our patients was 48.84 years, with extremes ranging from 31 to 67 years. The 45-50 age group was the most common.
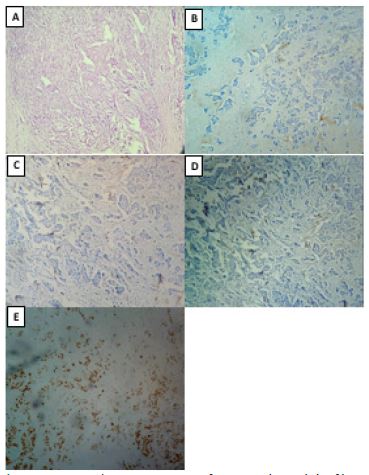
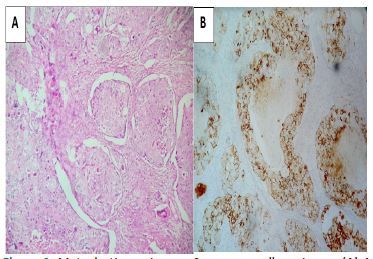
Clinical and para-clinical features: The most frequent reason for consultation in our patients was a breast nodule (82.7%), in the left breast in 60.60% and the right breast in 39.39% of cases. After conducting mammography on all our patients, we got the following results; according to the ACR (American College of Radiology) classification; ACR 5 in 57.14% of cases. ACR 4 in 42. 85%, with a mean lesion size of 28 mm. In 92, 15% of cases, the diagnosis of TNBC required an anatomopathological study of the biopsy. Histological features: the most frequent histological type was non-specific infiltrating carcinoma in 78% of cases (Figure 1), followed by metaplastic carcinoma in 20% (FigFigure 2) and adenoid cystic carcinoma in 2%. The Scarff-Bloom-Richardson (SBR) histopronostic grade for our patients was SBR III in 75.60%, SBR II in 21.95% and SBR I in 2%. Vascular emboli were present in 7.14%. On immunohistochemistry, ER and PR were absent in 100% of our patients, HER2 was 0 in 64.51%, 1 in 16.12% and 2 in 19.35%. In the latter case, an absence of HER2 oncogene amplification required a Chromogenic in Situ Hybridization (CISH) study. The Ki 67 proliferation index was assessed in all patients; with a rate >14% in 84.51% of cases (Figure 1E). All our patients underwent thoraco-abdominal CT scans and bone scans for extension assessment. At the end of this evaluation, we detected three metastatic localizations of breast cancer, two cases with pulmonary and bone metastases and another case with liver metastases.
TNM classification: According to the AJCC 2018 pTNM classification, our patients can be classified as follows:
Table 1: The course of endoscopic treatments.
| stage | Number | Percentage |
|---|---|---|
| I | 12 | 24 |
| IIA | 26 | 52 |
| IIB | 6 | 12 |
| IIIA | 1 | 2 |
| IIIB | 1 | 2 |
| IIIC | 1 | 2 |
| IV | 3 | 6 |
Discussion
At the 13th International Conference of the Expert Group on Breast Cancer in St. Gallen (2013), adopted clinic pathological and molecular definitions of breast carcinoma subtypes based on immunohistochemical characteristics of ER, PR, ERBB2 (HER2) and Ki-67 [6]. They were as follows: Luminal A-like, Luminal B-like (HER2-negative), Luminal B-like (HER2-positive), HER2-positive (non-luminal), and Triple-negative. In 2011, Lehmann et al. classified TNSCs into six subtypes using gene expression profiling on tumor samples from 587 TNSC patients: Basal-Like 1 (BL1), Basal-Like 2 (BL2), Mesenchymal (M), Mesenchymal Stem-Like (MSL), Immunomodulatory (IM) and Luminal Androgen Receptor (LAR) [8]. This new classification has made it possible to adapt the therapeutic management of TNBC. Depending on the series published in the literature, TNBC accounts for 10 to 25% of invasive breast cancers [7]. In our series, it represented 11.87%. The prevalence of TNBC appears to be higher in African-American women than in Caucasian women, with the age of onset often under 50 or even under 40 [8]. In our series, the age group most affected was 45-50. TNBC is often associated with a family history of breast cancer, essentially linked to BRCA1 gene mutation [9,10]. Histologically, TNBC is highly heterogeneous, with non-specific infiltrating carcinoma accounting for the majority in 70-80% of cases [11]. However, some TNBC have a favorable prognosis, namely adenoid cystic carcinoma, secretory carcinoma, and medullary carcinoma [12,13]. This is not the case for metaplastic carcinomas, which have a poor prognosis, particularly in high-grade cases [13]. In our series, non-specific infiltrating carcinoma was the most frequent histological type, accounting for 80%. On immunohistochemistry, high Ki67 is generally a sign of a poor prognosis. However, this high rate observed in the majority of TNBC is in favor of a better response to Neoadjuvant chemotherapy [14]. Therapeutic management relies on surgery, which remains the treatment of choice, combined with loco regional adjuvant radiotherapy and systemic chemotherapy. The high mitotic index in TNBC gives it greater chemosensitivity, and a high rate of histological complete histological remission after Neoadjuvant chemotherapy [15]. The heterogeneity and molecular complexity of TNBC explains the heterogeneity of response to chemotherapy, making it essential to study the phenotype of this type of cancer in order to tailor chemotherapy. The presence of multiple molecular alterations that could represent potential therapeutic targets, has led to the search for targeted therapies that are currently undergoing clinical trials, such as PARP (poly (ADP-ribose) polymerase) and EGFR inhibitors, anti-angiogenic agents and antiandrogens [16,17], and immunotherapy, which also represents one of the new therapeutic alternatives for TNBC. However, because of its rapid progression, TNBC has a poor prognosis in non-responders, despite its chemosensitivity. The main limitations of our work were: the small sample size, the retrospective nature of the study and the absence of a molecular study, so it limited the objective assessment of clinical evolution and post treatment survival. Our work has enabled us to take stock of the main epidemiological and clinicopathological features of TNBC at our facility, with a review of the literature concerning the molecular profile and recent therapeutic approach.
Conclusion
The results of our study are consistent with the literature on the epidemiological and clinicopathological aspects of TNBC. Triple-Negative Breast Cancer (TNBC) is a clinically, morphologically, molecularly and prognostically heterogeneous subgroup of breast cancer, requiring multidisciplinary collaboration and the search for new avenues of targeted therapy to optimize its management.
Declarations
Acknowledgements: Not applicable.
Conflict of interest: No conflicts of interest.
Funding statement: This study was not funded.
Ethical approval: Not applicable.
Consent for publication: Written informed consent was obtained from the patients for publication of this study and accompanying images. A copy of the written consents is available for review by the Editor-in-Chief of this journal on request.
Declaration of competing interest: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Availability of data and materials: Not applicable.
Author’s contributions: IE and YB analyzed and interpreted the patient data and wrote the manuscript. IE and DB made the figures. IE performed the histological examination. MO and JK proposed the study, supervised IE and revised the manuscript. All authors read and approved the final manuscript.
Registration of research studies: Not applicable.
References
- Fourati A, Boussen H, El May M, Goucha A, Dabbabi B, et al. Descriptive analysis of molecular subtypes in Tunisian breast cancer. Asia-Pacific Journal of Clinical Oncology. 2012; 10: e69-e74.
- Belkacémi Y, et al. Epidemiology of breast cancer in young women in North Africa. 32° Journées de la Société Française de Sénologie et de Pathologie Mammaire. Journées, Strasbourg, FRA, 2010-11-03: La femme jeune face au cancer du sein (Strasbourg, 3-5 novembre 2010) /Young woman facing breast cancer. 2010.
- Jemal A, et al. Global cancer statistics. CA: A cancer journal for clinicians, 2011; 61: 69-90.
- Furlanetto J, Loibl S. Optimal systemic treatment for early triple-negative breast cancer. Breast Care. 2020; 15: 217-226.
- Tan P, Ellis I, Allison K, Brogi E, Fox S, et al. The 2019 World Health Organization classification of tumours of the breast. Histopathology. 2020; 77: 181-185.
- Untch M, Gerber B, Harbeck N, Jackisch C, Marschner N, et al. 13th St Gallen international breast cancer conference 2013: Primary therapy of early breast cancer evidence, controversies, consensus-opinion of a German Team of Experts (Zurich 2013). Breast Care. 2013; 8: 1-1.
- Carey LA, Perou CM, Livasy CA, Dressler LG, Cowan D, et al. Race, breast cancer subtypes, and survival in the Carolina breast cancer study. JAMA. 2006; 295: 2492-502.
- Bauer KR, Brown M, Cress RD, Parise CA, Caggiano V. Descriptive analysis of Estrogen Receptor (ER)-negative, Progesterone Receptor (PR)-negative, and HER2-negative invasive breast cancer, the so-colled triple-negative phenotype: A population-based study from the California cancer registry. Cancer. 2007; 109: 1721-28.
- Trivers KF, Lund MJ, Porter PL, Liff JM, Flagg EW, et al. The epidemiology of triplenegative breast cancer, including race. Cancer Causes Control. 2009; 20: 1071-82.
- Cutuli B, Cohen Solal le Nir C, de Lafontan B, Mignotte H, Fichet V, et al. Breastconserving therapy for ductal carcinoma in situ of the breast: The French Cancer Centers´ experience. International Journal of Radiation Oncology Biology Physics. 2002; 53: 868- 879.
- Michy T, Le Bouëdec, Mishellany F, Penault Llorca F, Dauplat J. Existe-t-il encore une place pour l´examen extemporané dans le cancer du sein. Gynécologie obstétrique & fertilité. 2006; 34: 115-119.
- Rijani M, G Mac Grogan. Anatomie pathologie du sein. Encycl Med Chir. 1998.
- Vincent Salomon A, Macgrogan G, Charaffe Jauffret E, Jacquemier J, Arnould L. Identification of basal-like carcinomas in clinical practice: “Triple zero/BRCA1-like” carcinomas. Bulletin du cancer. 2010; 97: 357-363.
- Yerushalmi R, Woods R, Ravdin PM, Hayes MM, Gelmon KA. Ki67 in breast cancer: Prognostic and predictive potential. Lancet Oncol. 2010; 11: 174-83.
- Carey LA, Dees EC, Sawyer L, Gatti L, Moore DT, et al. The triple negative paradox: Primary tumor chemosensitivity of breast cancer subtypes. Clin Cancer Res. 2007; 13: 2329-34.
- Perou C M. Molecular stratification of triplenegative breast cancers. The Oncologist. 2011; 16: 61-70.
- Ashworth A. A synthetic lethal therapeutic approach: Poly (ADP) ribose polymerase inhibitors for the treatment of cancers deficient in DNA double-strand break repair. J Clin Oncol. 2008; 26: 3785-90.