
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Complicated extra pulmonary genitourinary tuberculosis in a teenager: A rare case report
Gashaw Arega1*; Meklit Deju1; Fathia Omer2; Leul Adane2
1Department of Pediatrics and Child Health, Tikur Anbessa Hospital, Addis Ababa University, Addis Ababa, Ethiopia.
2Department of Radiology, Tikur Anbessa Hospital Addis Ababa University, Addis Ababa, Ethiopia.
*Corresponding Author : Gashaw Arega
Department of Pediatrics and Child Health, Tikur Anbessa Hospital, Addis Ababa University, Addis Ababa, Ethiopia.
Email: gashawarega@gmail.com
Received : Dec 27, 2023
Accepted : Jan 12, 2024
Published : Jan 19, 2024
Archived : www.jcimcr.org
Copyright : © Arega G (2024).
Abstract
Genitourinary tuberculosis is a rare manifestation of extrapulmonary tuberculosis in children with vague symptoms and clinical presentations. It may be complicated with obstruction, and urethral stricture, and may lead to chronic renal disease if not diagnosed and treated promptly. We report the case of a 13-year-old male adolescent, we report a 13-year-old male adolescent who presented with difficulty urination and flank pain. He didn’t have close contact with tuberculosis-diagnosed patients. Abdominopelvic CT scan showed thickening and enhancement of the ureter and obstruction at the level of the ureter vesical junction, and multiple small hypoechoic bilateral renal parenchymal lesions. A Voiding Cyst Urethrogram (VCUG) and Doppler ultrasound showed a bulbous urethral stricture, and an aortic thrombus extending from the origin of the superior mesenteric artery to the left renal artery respectively. The urinary GeneXpert MTB/RIF and the Lateral Flow urine Lipoarabinomannan (LF‐LAM) assay for active tuberculosis were positive. We presented this complicated extrapulmonary tuberculosis case with ureteral stenosis, urethral stricture, and an aortic thrombus which was managed successfully with anti-tuberculosis medical therapy without surgical intervention.
Keywords: Genitourinary tuberculosis; VCUG; LF-LAM; GeneXpert; Anti-tuberculosis; Case report.
Citation: Arega G, Deju M, Omer F, Adane L. Complicated extra pulmonary genitourinary tuberculosis in a teenager: A rare case report. J Clin Images Med Case Rep. 2024; 5(1): 2808.
Case presentation
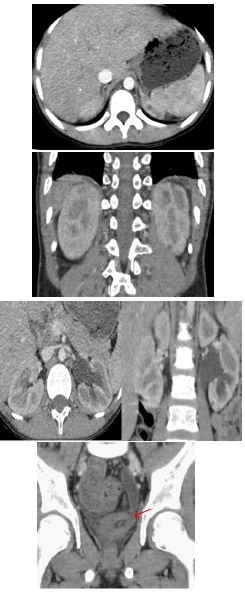
A 13-year-old male adolescent presented with a complaint of a gradual onset of difficulty in passing urine of eight months duration associated with a poor stream followed by post-voiding dribbling. After two months, his symptoms were accompanied by a colicky type of left flank pain. For the above complaint, he was taken to the nearby General Hospital where he was investigated with urinalysis, abdominal ultrasound, and voiding cystourethrogram. He was diagnosed with left hydronephrosis with obstruction at the level of left UVJ, and Urinary Tract Infection (UTI). He was treated with unspecified PO medications and was on follow-up every two weeks. Later he had a diagnostic ureteroscopy, and J-stent insertion was done to relieve the obstruction as his creatine level increased to 1.4 gm/dl. One day after the procedure he developed a high-grade fever and decreased urine output. J-stent was removed with consideration of stent failure. Suprapubic cystostomy was done for acute urinary retention secondary to urethral stricture and subsequently, he was treated with multiple IV antibiotics for complicated pyelonephritis. Chest X-ray and sputum analysis for tuberculosis workup were negative. Later he was referred to our tertiary center for better investigations and management. A general physical examination showed a well-grown male adolescent with stage II hypertension and unaffected anthropometry. The pertinent systemic physical examination was on the genitourinary system; there was a suprapubic cystostomy Foley catheter in situ with a mild left Costovertebral Angle (CVA) and suprapubic tenderness. Urine analysis, renal function was normal, with a creatine level of 0.5 mg/dl, and chest x-ray was unremarkable. Abdominal pelvic CT scan showed a left mild hydroureteronephrosis with distal narrowing at the vesicoureteral junction. There are multiple small hypoechoic bilateral renal parenchymal lesions and a thick irregular-walled collapsed urinary bladder with a suprapubic catheter in place (Figure 1).
The Voiding Cyst Urethrogram (VCUG) from the referral showed a proximal urethral dilatation with a smooth outline. There is abrupt narrowing at the proximal bulbous portion; only a thin track of voiding contrast passing suggestive of a bulbous urethral stricture, with an estimated length of stricture of less than 5 mm (Figure 2).

Doppler ultrasound showed an aortic thrombus extending from the origin of the superior mesenteric artery to the left renal artery with an oscillating nature transiently and partially occluding the main left renal artery, and echocardiography was normal. The urinary GeneXpert MTB/RIF and the Lateral Flow urine Lipoarabinomannan (LF‐LAM) assay for tuberculosis were positive. The child was started with anti-tuberculosis with a 2RHZE/4RH regimen (Rifampicin, Isoniazid, Payrazianmide, and ethambutol), nifedipine for hypertension, and anticoagulation with enoxaparin was started for the aortic thrombus, and continued with warfarin and aspirin for four months. The urinary GeneXpert after the 2 months of the intensive phase of anti-tuberculosis treatment turned out to be negative and the continuation phase of treatment continued for four months. Abdomino-pelvic ultrasound was normal while treatment was completed, and the child was declared cured without chronic complications. The urethral stricture, ureteral stenosis, and aortic thrombus resolved without surgical interventions.
Discussion
Tuberculosis is a major health problem in developing countries. Urinary tract TB is a rare disease in children and represents less than 5% of childhood extra pulmonary tuberculosis presented with vague symptoms and signs [1-4].
Diagnosing genitourinary tuberculosis is challenging in highly TB-endemic low-income countries, and the chance of underdiagnosis is high. Urinary tract tuberculosis has a wide spectrum of presentations, ranging from pain on micturition and hematuria to complicated forms such as acute renal failure, staghorn calculus, pyonephrosis, urethral stricture, contracted bladder, and chronic kidney disease [2,5-9]. The genitourinary involvement in tuberculosis can be part of a disseminated infection or a localized genitourinary disease [9-11]. The dissemination of infection to the kidney and renal pelvis can cause tuberculous pyelonephritis. The tubercle bacilli can easily disseminate from the ureter to the bladder, causing granulomatous lesions associated with fibrosis, causing a series of ureteral dilations intercalated with strictures, and segmental stenosis leading to urinary obstruction and urine reflux causing hydroureteronephrosis [11-13]. The diagnosis of urinary tract TB is based on urine analysis, diagnostic imaging with abdominal ultrasound and CT scan, acid-fast bacilli culture, and molecular diagnosis of TB using urinary GeneXpert MTB/RIF and the Lateral Flow urine Lipoarabinomannan (LF‐LAM) [13,18,19]. Imaging has an important role in making early diagnosis and treatment, although cultures or histologic analysis is required for definitive diagnosis. Imaging in renal TB depends upon the extent and stage of the disease process. Intravenous Urogram (IVU) is the gold standard imaging modality for early diagnosis of GU tuberculosis for demonstration of fine erosive changes that affect the urothelium [20,21]. Currently, available Multidetector Computed Tomography (MDCT) scanners offer much better CT programs, and most findings on an IVU are being detected on CTU. The most valuable feature of renal TB is the multiplicity of abnormal findings CT features of renal TB result from a combination of parenchymal and collecting system lesions. Early changes in renal TB include granulomas of ≤3 mm in size and papillary necrosis, multifocal strictures affecting any part of the collecting system hydronephrosis, mural thickening, and enhancement are seen as part of progressive disease, and progressive hydronephrosis results in very thin parenchyma and amorphous dystrophic calcification eventually involve the entire kidney (known as a putty kidney) as an end-stage disease [21].
Our patient had multiple fine hypo-enhancing bilateral cortical nodules and irregular multifocal urothelial thickening with enhancement and moderated hydronephrosis considering the epidemiology and clinical background tuberculosis is considered and is conformed with molecular testing. The cornerstone treatment of genitourinary tuberculosis is anti-tuberculosis therapy. Treatment for 6 months is recommended for urinary tuberculosis; 2HRZE in the first 2 months; isoniazid (H), Rifampicin (R), pyrazinamide (Z), and Ethambutol (E) followed by isoniazid and rifampicin for four months (4HR) [8,15-17].
Our patient was diagnosed with extrapulmonary genitourinary tuberculosis radiologically, and confirmed with urinary GeneXpert MTB/RIF and the Lateral Flow urine Lipoarabinomannan (LF‐LAM) assay. He was treated with 2HRZE/4H anti-tuberculosis therapy and declared cured after he took the treatment for six months. He is doing well on follow-ups without having any chronic complication sequelae.
Conclusion
A high index of suspicion of genitourinary tuberculosis is necessary in TB-endemic countries. A wide range of investigations may be required to achieve a complete diagnosis of urinary tract tuberculosis including diagnostic imaging, urinary GeneXpert MTB/RIF, and the Lateral Flow urine Lipoarabinomannan (LF‐LAM) molecular assay to early diagnose and avoid complications.
Declarations
Ethical approval: This study was approved by the research and ethics committee of the Department of Pediatrics, School of Medicine, Addis Ababa University.
Parental consent: Written informed consent was obtained from the patient’s parents for publication and any accompanying images.
Acknowledgments: We express special thanks to the parents of the child for giving consent to publish this report for academic purposes.
Financial support and sponsorship: Nil.
Conflicts of interest: Nil.
References
- Nataprawira HM, Pratama AA, Widiasta A, et al. Complicated Urinary Tract Tuberculosis in a 13-year-old Adolescent with Chronic Kidney Disease and Antituberculous Drug-Induced Hepatotoxicity. Case Rep Infect Dis. 2019; 2019: 7370150.
- Chattopadhyay A, Bhatnagar V, Agarwala S, Mitra DK. Genitourinary tuberculosis in pediatric surgical practice. J Pediatr Surg. 1997; 32: 1283-6.
- Nataprawira HM, Hannah RA, Kartika HH. Hospitalized pediatric antituberculosis drug-induced hepatotoxicity: Experience of an Indonesian referral hospital. Asian Pacific Journal of Tropical Disease. 2017; 7: 276-279.
- Feigin RD, Cherry JD, Demmler GJ, Kaplan SL. Textbook of Pediatric Infectious Diseases. Philadelphia, PA, USA: Saunders. 1981.
- WHO. Global Tuberculosis Report 2017. Geneva, Switzerland: WHO. 2017.
- Abbara A, Chitty S, Roe JK, et al. Drug-induced liver injury from antituberculous treatment: A retrospective study from a large TB center in the UK. BMC Infectious Diseases. 2017; 17: 231.
- Ramappa V, Aithal GP. Hepatotoxicity related to anti-tuberculosis drugs: Mechanisms and management. Journal of Clinical and Experimental Hepatology. 2013; 3: 37-49.
- Gupta SD, Das P, Ahuja A. Incidence, etiopathogenesis and pathological aspects of genitourinary tuberculosis in India: A journey revisited. Indian Journal of Urology. 2008; 24: 356.
- Muttarak M, Chiang Mai WN, Lojanapiwat B. Tuberculosis of the genitourinary tract: Imaging features with pathological correlation. Singapore Med J. 2005; 46: 568-574.
- Eastwood JB, Corbishley CM, Grange JM. Tuberculosis and the kidney. J Am Soc Nephrol. 2001; 12: 1307-1314.
- Yarger WE. The urinary tract is obstructive. In: Brenner BM, Rector FC, editors. The Kidney. Fourth edition. Saunders: Philadelphia/London: W.B. Saunders. 1991; 1768-1808.
- Mandell GL, Bennett JE, Dolin R. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 7th ed. Philadelphia, PA: Churchill Livingstone Elsevier. 2010; 2010.
- Daher Ede F, da Silva GB, Barros EJ. Renal tuberculosis in the modern era. Am J Trop Med Hyg. 2013; 88: 54-64.
- Daher Ede F, da Silva GB, Barros EJ. Renal tuberculosis in the modern era. Am J Trop Med Hyg. 2013; 88: 54-64.
- Kulchavenya E. Best practice in the diagnosis and management of urogenital tuberculosis. Therapeutic Advances in Urology. 2013; 5: 143-151.
- Kulchavenya E. Current Therapy and Surgery for Urogenital Tuberculosis. Berlin, Germany: Springer; 2016. Urogenital tuberculosis-definition, and classification. 2016; 31-49.
- Çek M, Lenk S, Naber KG, et al. EAU guidelines for the management of genitourinary tuberculosis. European Urology. 2005; 48: 353-362.
- Oliveira JL, Silva Junior GB, Daher EF. Tuberculosis-associated chronic kidney disease. Am J Trop Med Hyg. 2011; 84: 843-844.
- Lima NA, Vasconcelos CC, Filgueira PH, Kretzmann M, Sideaux TA, et al. Review of genitourinary tuberculosis with a focus on end-stage renal disease. Rev Inst Med Trop Sao Paulo. 2012; 54: 57-60.
- Becker JA. Renal tuberculosis. Urol Radiol. 1988; 10: 25-30.
- Merchant S, Bharati A, Merchant N. Tuberculosis of the genitourinary system-Urinary tract tuberculosis: Renal Tuberculosis-Part I. Indian J Radiol Imaging. 2013; 23: 46-63.