
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Clinical application of fiberoptic bronchoscopy guided awake tracheal intubation in removal of internal fixation for cervical spine fracture: Case report
Lin Zeng*; Tuo Luo; Yusong Liu; Yali Chen
Shifang People’s Hospital, Shifang, Sichuan Province, China.
*Corresponding Author : Lin Zeng
Shifang People’s Hospital, Shifang, Sichuan Province, China.
Email: 343329636@qq.com
Received : Dec 30, 2023
Accepted : Jan 15, 2024
Published : Jan 22, 2024
Archived : www.jcimcr.org
Copyright : © Zeng L (2024).
Abstract
Background and objectives: When planning the management of a predicted difficult airway, it is important to determine which strategy will be followed. Using fiberoptic bronchoscopy is a major option in scenarios with factors suggesting difficult airway access. It is also indicated in rescue situations, when there is tracheal intubation failure with direct laryngoscopy. The purpose of this report is to demonstrate the efficacy of using fiberoptic bronchoscopy as the preferred device for patients after cervical spine fracture surgery with almost no neck mobility and difficult airways.
Case report: An 47 year-old female patient, 168 cm, 65 kg, ASA Physical Status II, Mallampati IV classification, was scheduled for internal fixation removal surgery for cervical spine fractures. Although the patient had a difficult airway, she showed no signs of respiratory failure or airway obstruction. After entering the room, provide oxygen through a nasal catheter with a flow rate of 2 L/min. After establishing a venous pathway and monitoring, intravenous infusion of dexmedetomidine with a load of 0.5 ug/kg was completed within 10 minutes. During airway preparation, always maintain the patient’s autonomous breathing. The anesthesiologist performed a transcricoid puncture on the patient and injected 3 mL of 2% lidocaine solution into the tracheal cavity. The whole mouth was sprayed with 2% lidocaine under the guidance of fiberoptic bronchoscope. An armored tube with a guide wire inside was used for tracheal intubation, performed on the first attempt with appropriate glottis visualization.
Conclusion: The fiberoptic bronchoscope occupies a prominent position in cases in which access to the airway is difficult. Fiberoptic bronchoscope guidance in awake endotracheal intubation for patients with difficult airway has the advantages of rapid, accurate, safe, high success rate and little damage. This can provide a new and effective method for the difficult airway management of these patients.
Keywords: Topical anesthesia; Fiberoptic bronchoscope; Intubation; Difficult airway.
Citation: Zeng L, Luo T, Liu Y, Chen Y. Clinical application of fiberoptic bronchoscopy guided awake tracheal intubation in removal of internal fixation for cervical spine fracture: Case report. J Clin Images Med Case Rep. 2024; 5(1): 2810.
Background
Difficult airways usually put patients at risk during induction of general anesthesia [1], which may lead to a high proportion of airway related complications and mortality [2,3]. If conventional intubation is performed for patients with limited head movement after cervical spine fracture internal fixation, the position of the catheter front end can only be adjusted by moving or rotating the catheter, which may take a long time. Such patients are prone to intubation failure or even ventilation difficulties after conventional anesthesia induction. The mask ventilation we commonly use can provide patients with necessary oxygen supply. If the mask ventilation is difficult, it will endanger patients’ lives. In addition, the limited amplitude of head retroversion and epiglottis ptosis will make the airway between oropharynx and trachea appear “S” shape. If a catheter with a similar inner diameter to the trachea is used for blind intubation, the front end of the catheter will be difficult to align with the larynx or slide into the esophagus when exiting the catheter core and rotating and pushing the catheter. This not only reduces the success rate of intubation, but also easily causes complications, such as local injury, bleeding, cough, laryngeal edema, bronchospasm and postoperative hoarseness. During anesthesia, the management of difficult airways has been challenging and related to the safety and quality of anesthesia [4]. Many serious anesthesia related complications are caused by improper airway management. Awake endotracheal intubation guided by fiberoptic bronchoscope is a safe and effective method to manage difficult airways. However, patients must experience intolerable pain when undergoing intubation while fully awake. Ovassapian believed that conscious sedation could partly improve their tolerability, though he stressed the importance to avoid respiratory depression whenever possible during endotracheal intubation, as it would be directly linked with the safety of anesthesia [5]. At the same time, for patients with a history of cervical spine fracture, preventing severe cough is helpful to reduce the risk of further cervical spine injury [6]. Increasing the dose of sedatives can undoubtedly improve the tolerance of endotracheal intubation, but it also greatly increases the risk of excessive sedation and respiratory depression. In addition, although conscious sedation is important for intubation tolerance, the dose recommended in some studies is still insufficient to produce a depth of anesthesia that eliminates airway reactivity after intubation. Therefore, the main method to avoid cough reaction during awake tracheal intubation should be adequate airway surface anesthesia. The main purpose of conscious sedation is to eliminate or reduce the discomfort during airway surface anesthesia and intubation.
We introduce a case to observe the effect of intraoral awake intubation with fiberoptic bronchoscope in patients after cervical fracture internal fixation. To the best of our knowledge, this study is the first to report the perioperative airway management of a patient with a history of cervical fracture internal fixation surgery combined with difficult airway.
Case presentation
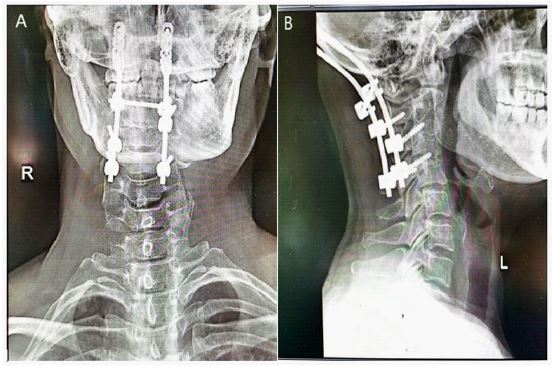
A 47 year old woman with a Body Mass Index (BMI) of 23.03 kg/m2 was planned to undergo removal of cervical internal fixation under general anesthesia with endotracheal intubation. The patient fell from a high place 17 months ago, resulting in comminuted fractures of C3 and C4 vertebral bodies, and underwent open reduction and internal fixation in our hospital (Figure 1). Airway examination revealed a short neck, Mallampati IV classification due to limited cervical and mandibular mobility. The patient was scheduled for elective surgery on September 11, 2023. After general anesthesia induction, the operation was suspended due to failure of conventional intubation. So on September 15, 2023, it was planned to undergo elective surgery again.
We choose to perform fiberoptic bronchoscope guided endotracheal intubation after sedation and surface anesthesia to maintain the patient’s spontaneous breathing to avoid hypoxia. After the patient entered the room, the venous access was opened and the nasal catheter was given for oxygen inhalation, electrocardiogram, blood pressure and blood oxygen saturation (SpO2) were monitored, and the left radial artery puncture pressure was measured under local anesthesia. Patients were given intravenous dexmedetomidine 0.5 μg/kg pump injection for 10 min. Then the patient was given lidocaine aerosol (tachyptol) to spray the throat twice every 5 min. After the puncture of cricothyroid membrane, 3 ml of 2% lidocaine was given, and then the endotracheal intubation was guided by fibro bronchoscope. Before intubation, tetra Caine mucilage was applied to the endotracheal tube (ID7.0 reinforced tube). Before intubation, a fiberoptic bronchoscope was inserted into the endotracheal tube. When the fibro bronchoscope crossed the epiglottis to expose the glottis, the patient was given 3 ml of 2% lidocaine for glottic surface anesthesia within the field of view of the fibro bronchoscop. The patient was instructed to inhale deeply. When the glottis of the patient was open, the top of the fiberoptic bronchoscope was sent to the place 3-5 cm away from the carina, and then the patient was given 2% lidocaine 3 ml through the fiberoptic bronchoscope for surface anesthesia of the main trachea. After topical anesthesia, the anesthesiologist pushed the catheter into the trachea, and withdrew from the fibro bronchoscope after determining the catheter position. The cuff was inflated and fixed after exiting the bronchoscope, and the endotracheal tube was connected to the anesthesia machine for oxygen inhalation. Propofol 130 mg, midazolam 2 mg, sufentanil 20 ug and CIS atracurium 10 mg were immediately injected intravenously. Then continue to pump propofol 400 mg/h and remifentanil 390 ug/h for anesthesia maintenance. After the patient’s spontaneous breathing disappeared, the anesthesia machine was used to control breathing. After 1.2 hours, the operation was successfully completed. The tracheal tube was removed after the patient was awake. The patient was transferred to the anesthesia recovery room and returned to the ward without abnormality after 30 min of observation.



Discussion
For anticipated difficult airways, preserving autonomous breathing intubation is crucial for difficult airway intubation [7]. Previous studies have shown that traditional laryngoscopes and light sticks cannot completely solve difficult airway problems [8]. Fiberoptic bronchoscopy guided conscious tracheal intubation is a safe method to avoid difficulties in ventilation and intubation after the use of general anesthesia drugs [9]. During fiberoptic bronchoscopy intubation, the display is clear, the intubation is accurate, and the success rate is high. However, in a conscious state, intubation stimulation can cause patients to cough, suffocate, have spasms in the throat and bronchi, fluctuate circulation, and even cause severe arrhythmia or cardiac arrest [10]. Therefore, a good surface anesthesia effect is the key to ensuring the success of conscious tracheal intubation guided by fiberoptic bronchoscopy. Studies have shown that intravenous infusion of drugs such as dexmedetomidine before conscious intubation can effectively suppress adverse reactions during tracheal intubation in patients [11]. The patients in this study had a history of cervical spine fracture internal fixation surgery. The patient’s head and neck cannot be rotated, bent, or extended. In addition, the patient’s neck was flexed forward and his mouth was limited due to the internal fixation surgery. Mallampati grade IV of this patient is also noteworthy [12]. In this case, an experienced anesthesiologist performed awake endotracheal intubation on the patient.
In this study, dexmedetomidine was given by syringe pump to relieve the anxiety of patients. In order to maximize the success rate of awake endotracheal intubation with the minimum amount of sedative drugs, the upper airway must be fully surface anesthetized. Some researchers reported the use of customized nebulizers to spray the oropharyngeal airway, which provided effective local airway anesthesia and optimized patient comfort [13]. Therefore, we used a sprayer to perform tracheal surface anesthesia, and percutaneous injection of 2% lidocaine from the middle line of the cricothyroid membrane to the trachea cavity. In addition, the root of tongue, oropharynx, hypopharynx and pharyngeal structures were surface anesthetized with 2% lidocaine by using a fibrobronchoscope visualization method. After satisfactory superficial anesthesia, awake endotracheal intubation was performed using a fiberoptic bronchoscope. Due to the good cooperation of the patients, the clinical effect of intubation was satisfactory. It was found that patients undergoing surgery were more likely to recover from total intravenous anesthesia with propofol and dexmedetomidine than from inhalation anesthesia [14]. Intraoperatively, we avoided the use of volatile anesthetics because of the risk of malignant hyperthermia, which occurs in genetically susceptible individuals with a high metabolic response to potent inhaled anesthetics or succinylcholine [15]. In this case, total intravenous anesthesia was used to induce and maintain, and the anesthetic dose was strictly calculated and actively adjusted according to the depth of anesthesia. The patient woke up 5 minutes after operation and stayed in PACU for 30 minutes. Unfortunately, we had no access to sugammadex, so instead, we used neostigmine for muscle relaxant reversal. Studies have shown that administering sugammadex according to a patient’s ideal body weight leads to faster reversal and is independent of relapse. A previous study supports dosing sugammadex according to ideal body weight regardless of the depth of neuromuscular blockage or type of neuromuscular blocker [16]. We speculate that the use of sugammadex could reduce the PACU time. It has been reported that adding midazolam or propofol before awake tracheal intubation may have a better amnestic effect [17,18]. These drugs were not used in this study because we wanted to ensure safety and patients were fully awake so that we could determine the sedative effect of dexmedetomidine during awake tracheal intubation. Although the patient was aware of intubation, this study showed that she was satisfied with the whole anesthesia process and had no other adverse reactions. In addition, because the dose range of dexmedetomidine used in this study is only for clinical reference, further studies based on larger samples are needed to determine the optimal value of awake intubation.
Conclusion
In this paper, we discuss the successful application of fiberoptic bronchoscope guided awake intubation in surgical patients with limited cervical mobility and difficult airway. This approach should be considered for patients with similar conditions.
Declarations
Acknowledgements: Not applicable.
Funding: The authors declare that they have no funding.
Availability of data and materials: All attainable data are within in the paper and (Figure 1). All data are fully available without restriction.
Authors’ contributions: Lin Zeng, Tuo Luo, Yusong Liu and Yali Chen participated in data collection and analysis. Lin Zeng drafted the manuscript, Tuo Luo designed the study. All authors approved the final version of the manuscript.
Ethics approval and consent to participate: A local ethics committee ruled that no formal ethics approval was required in this particular case.
Consent for publication: Written informed consent was obtained from the patient for publication.
Competing interests: There are no competing interests amongst the authors and there is not going to be any forthcoming presentation.
References
- Peng J, Ye J, Zhao Y, Liang J, Huang H, et al. Supraglottic jet ventilation in difficult airway management. J Emerg Med. 2012; 43: 382-90.
- Fritzsche K, Osmers A. Anästhesiologische Besonderheiten bei der laryngotrachealen Chirurgie. Hochfrequenzjetventilation als spezielle Beatmungsstrategie während der Narkose. Anesthetic management in laryngotracheal surgery. High-frequency jet ventilation as strategy for ventilation during general anesthesia. Anaesthesist. 2010; 59: 1051-61.
- Leiter R, Aliverti A, Priori R, Staun P, Lo Mauro A, et al. Comparison of superimposed high-frequency jet ventilation with conventional jet ventilation for laryngeal surgery. Br J Anaesth. 2012; 108: 690-7.
- Braz LG, Braz DG, Cruz DS, Fernandes LA, Módolo NS, et al. Mortality in anesthesia: A systematic review. Clinics (Sao Paulo). 2009; 64: 999-1006.
- Ovassapian A. The flexible bronchoscope. A tool for anesthesiologists. Clin Chest Med. 2001; 22: 281-99.
- Wang SY, Mei Y, Sheng H, Li Y, Han R, et al. Tramadol combined with fentanyl in awake endotracheal intubation. J Thorac Dis. 2013; 5: 270-7.
- Ahmad I, El Boghdadly K, Bhagrath R, Hodzovic I, McNarry AF, et al. Difficult Airway Society guidelines for Awake Tracheal Intubation (ATI) in adults. Anaesthesia. 2020; 75: 509-528.
- Rouby JJ, Arbelot C, Gao Y, Zhang M, Lv J, et al. APECHO Study Group. Training for Lung Ultrasound Score Measurement in Critically Ill Patients. Am J Respir Crit Care Med. 2018; 198: 398-401.
- Pandya S, Baser O, Wan GJ, Lovelace B, Potenziano J, et al. The Burden of Hypoxic Respiratory Failure in Preterm and Term/Near-term Infants in the United States 2011-2015. J Health Econ Outcomes Res. 2019; 6: 130-141.
- Roberts CL, Badgery Parker T, Algert CS, Bowen JR, Nassar N. Trends in use of neonatal CPAP: A population-based study. BMC Pediatr. 2011; 11: 89.
- Ahmad KA, Bennett MM, Ahmad SF, Clark RH, Tolia VN. Morbidity and mortality with early pulmonary haemorrhage in preterm neonates. Arch Dis Child Fetal Neonatal Ed. 2019; 104: F63-F68.
- Mahmoud M, Hasanin AM, Mostafa M, Alhamade F, Abdelhamid B, et al. Evaluation of super-obesity and super-super-obesity as risk factors for difficult intubation in patients undergoing bariatric surgery. Surg Obes Relat Dis. 2021; 17: 1279-1285.
- Leung Y, Vacanti FX. Awake without complaints: Maximizing comfort during awake fiberoptic intubation. J Clin Anesth. 2015; 27: 517-9.
- Elbakry AE, Sultan WE, Ibrahim E. A comparison between inhalational (Desflurane) and total intravenous anaesthesia (Propofol and dexmedetomidine) in improving postoperative recovery for morbidly obese patients undergoing laparoscopic sleeve gastrectomy: A double-blinded randomised controlled trial. J Clin Anesth. 2018; 45: 6-11.
- Rüffert H, Bastian B, Bendixen D, Girard T, Heiderich S, et al. European Malignant Hyperthermia Group. Consensus guidelines on perioperative management of malignant hyperthermia suspected or susceptible patients from the European Malignant Hyperthermia Group. Br J Anaesth. 2021; 126: 120-130.
- Horrow JC, Li W, Blobner M, Lombard J, Speek M, et al. Actual versus ideal body weight dosing of sugammadex in morbidly obese patients offers faster reversal of rocuronium-or vecuronium-induced deep or moderate neuromuscular block: A randomized clinical trial. BMC Anesthesiol. 2021; 21: 62.
- Piepho T, Thierbach AR, Göbler SM, Maybauer MO, Werner C. Comparison of two different techniques of fibreoptic intubation. Eur J Anaesthesiol. 2009; 26: 328-32.
- Kim MK, Lee JW, Jang DJ, Shin OY, Nam SB. Effect-site concentration of remifentanil for laryngeal mask airway insertion during target-controlled infusion of propofol. Anaesthesia. 2009; 64: 136-40.