
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Progesterone induced renal cell carcinoma during pregnancy: A case report
Mohsen Sarkarian1; Negar Behtash2*; Mohammad Ali Afandy3
1Department of Urology, Golestan Hospital, Ahvaz Jundishapur University of Medical Sciences, Iran.
2Department of Urology, Ahvaz Jundishapur University of Medical Sciences, Iran.
3Department of Pathology, Ahvaz Jundishapur University of Medical Sciences, Iran.
*Corresponding Author : Negar Behtash
Department of Urology, Ahvaz Jundishapur University of Medical Sciences, Iran.
Email: negarbehtash@gmail.com
Received : Dec 30, 2023
Accepted : Jan 16, 2024
Published : Jan 23, 2024
Archived : www.jcimcr.org
Copyright : © Behtash N (2024).
Abstract
Diagnosis of cancer is rare during pregnancy and renal cell carcinoma appears to be the most common urological neoplasm in gestation. We presented a 29-year-old pregnant woman who was treated with progestogen for secondary infertility and developed renal mass during pregnancy.
Keywords: Renal cell carcinoma; Pregnancy; Partial nephrectomy.
Citation: Sarkarian M, Behtash N, Ali Afandy M. Progesterone induced renal cell carcinoma during pregnancy: A case report. J Clin Images Med Case Rep. 2024; 5(1): 2812.
Introduction
Renal cell carcinoma is a rare complication during pregnancy period. However literature revealed that kidney tumours are the most common urological neoplasm which were reported in pregnancy [1,2]. RCC in pregnant women could present with symptoms suggestive for other common disorders such as urinary tract infection [3]. In this article we reported a case of progesterone induced renal cell carcinoma which was discovered accidentally in a routine pregnancy exam.
Case presentation
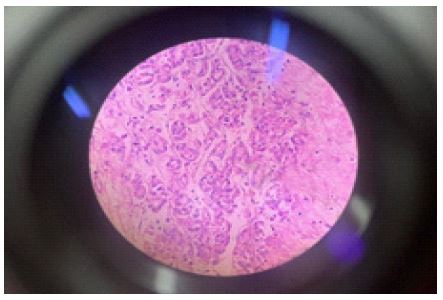
29-year-old woman G3P2Ab1 was referred to our clinic for evaluation of a huge right renal mass which was found accidental in routine pregnancy check-up program at 25 weeks of gestation. She had a normal vaginal delivery which resulted in a healthy baby 9 years ago and had therapeutic abortion due to foetus abnormalities 2 years ago. After the miscarriage she was unable to conceive, so she was evaluated for secondary infertility. Hypothyroidism was found in primary evaluations and Levothyroxine was prescribed. In addition, her haemoglobin level was 9.8 g/dl. Infertility treatment was continued with ASA and Progesterone (suppository and ampule). In routine follow up evaluation patient complained of dull right flank pain with no urinary tract symptoms. Kidney ultra sound revealed a lesion in lower pole of right kidney. Based on clinical symptoms and size of the lesion conservative management was considered and close follow up with sonography was planned. Unfortunately, control imaging revealed enlargement in mass size and finally, a large thick wall multilocular cystic lesion with fine internal echoes and scattered coarse calcification at lower pole of right kidney extending to midline accompanied with solid component was reported. The probable suspicions diagnosis was confirmed by following MRI imaging. After consultation with a multidisciplinary team, the patient was prepared for partial nephrectomy. Finally histopathological evaluation revealed renal cell carcinoma with no sarcomatoeid and rhabdomioeid feature and no tumour necrosis without lymphovascular invasion with Fuhrman nuclear grade 2 and clear surgical margin. Follow up kidney sonography one month after surgery was done and there was acceptable.

Discussion
Diagnosis of malignancies in course of pregnancy period is challenging clinical situation. In general, the incidence of renal cell carcinoma is about 3% of adult with slightly male predominance, but because pregnant women are excluded from clinical trials, the incidence of RCC remains unclear during pregnancy [4]. Breast cancer, cervical cancer, melanoma and lymphomas are the most frequent neoplasms which were reported during pregnancy. Literature reviews revealed renal tumours are the most common urological malignancy and adenocarcinoma is the most common type of kidney neoplasm during gestation [5]. Reproductive hormonal factors has mentioned in some studies but no direct dependency was find up till now [6]. Some researches demonstrated that elevated level of progesterone and oestrogen may increase risk of renal cell carcinoma in multiparous pregnant women in compared with nulliparous [7]. In our patient due to infertility treatment, additional progesterone was prescribed and there were no other risk factors for renal mass was found. However, some cases reported with classical triad of RCC, flank mass is the most frequent presentation of RCC during pregnancy. Moreover, sometimes RCC may be asymptomatic and discovered by accident. Gravid womb may obscure kidney mass and makes difficulty in diagnosis [8]. Ultrasonography is the most common imaging tools for finding abnormal renal mass in pregnancy. Due to teratogenic effect on foetus, the use of CT scan during gestation is limited. Therefore following MRI imaging after ultrasound may confirm the diagnosis in this situation [9]. A standard guideline for management of RCC in pregnancy is not available due to rarity of this diagnosis. So clinical decision and surgical plan should be determined indiindividually and a multi-disciplinary team work group is mandatory for this purpose. Loughlin et al suggested early surgical plan for tumour which was found in first trimester of gestation [10]. On the other hand, in second trimester surgical procedure may result in foetal distress or spontaneous labour. In addition, in third trimester resection of renal mass and caesarean section may be performed together or mass resection may be postponed until the labour [9]. Currently, termination of pregnancy should be considered in patient with metastatic tumour [11].
Open and laparoscopic surgical approach are available for renal mass resection and there are no statistical differences between complications after those techniques. Fortunately, most pregnant patients with RCC have acceptable prognosis and the pregnancy could result in healthy newborns. But there is no relevant data about prognosis of pregnant women with metastatic renal cell carcinoma [4,12]. Additional treatment may need for patient with advance disease.
Conclusion
Renal mass is an extremely rare disorder during pregnancy and could presented with various feature. There is no uniform management plan for this issue and decision making should be individual based on the patient’s situation. The overall prognosis of pregnant women with kidney mass is good but further investigation is still necessary to evaluate the risk of this problem for pregnant patients and their foetus.
References
- Walker JLE, L Knight. Renal cell carcinoma in pregnancy. Cancer. 1986; 58: 2343-2347.
- Boukhannous I, et al. Fast growing papillary renal cell carcinoma in first trimester pregnancy with postoperative inferior vena cava thrombosis: A case report. Urology Case Reports. 2020; 33: 101292.
- Gladman M, et al. Renal cell carcinoma in pregnancy. Journal of the Royal Society of Medicine. 2002; 95: 199-201.
- Khaled H, NAl Lahloubi, N Rashad. Review on renal cell carcinoma and pregnancy: A challenging situation. Journal of Advanced Research. 2016; 7: 575-580.
- Boussios S, N Pavlidis. Renal cell carcinoma in pregnancy: A rare coexistence. Clinical and Translational Oncology. 2014; 16: 122-127.
- Chow WH, LM Dong, SS Devesa. Epidemiology and risk factors for kidney cancer. Nature Reviews Urology. 2010; 7: 245-257.
- Yilmaz E, et al. Renal cell carcinoma diagnosed during pregnancy: A case report and literature review. Journal of International Medical Research. 2018; 46: 3422-3426.
- Akpayak I, et al. Renal cell carcinoma in pregnancy: Still a management challenge. African Journal of Urology. 2015; 21: 167-170.
- Csaba Berczi M, M Tibor Flasko. Renal Tumor in Pregnancy: A Case Report and Review of the Literature. 2017; 99: 367-369.
- Loughlin K. The management of urological malignancies during pregnancy. British journal of urology. 1995; 76: 639-644.
- David RA, et al. Peculiarities and management challenges of advanced renal cell carcinoma incidentally discovered in pregnancy. Clinical Case Reports. 2018; 6: 863.
- Xu H, S Tan. Diagnosis and treatment of renal cell carcinoma during pregnancy. Cancer Management and Research. 2021; 9423-9428.