
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Hirschsprung disease with recurrent obscure gastrointestinal bleeding
*Corresponding Author : Sayan Malakar
Department of Medicine, Dr RPGMC, Tanda, Kangra, HP, India.
Email: oneandonlydrsayan@gmail.com
sayan20sgpgi@gmail.com
Received : Dec 28, 2023
Accepted : Jan 16, 2024
Published : Jan 23, 2024
Archived : www.jcimcr.org
Copyright : © Malakar S (2024).
Citation: Malakar S. Hirschsprung disease with recurrent obscure gastrointestinal bleeding. J Clin Images Med Case Rep. 2024; 5(1): 2813.
Description
Hirschsprung Disease (HD) is a form of colonic aganglionosis with an incidence of 1 in 5000 liver births. It presents as constipation since birth with other intestinal and extraintestinal disorders [1]. Here we present a case of a 22-year-old female who presented with constipation since birth and repeated episodes of melena requiring a total of eight units of blood transfusion for the last six years. There was a history of prolonged defecation and digital evacuation of stool. For constipation, she was receiving sodium picosulfate, prucalopride and polyethylene glycol. As her symptoms were refractory, she was referred to us. On presentation, her hemoglobin was 6.3 grams/deciliter. As her esophagogastroduodenoscopy, ileo-colonoscopy, and abdominal imaging were normal, we kept the possibility of suspected small bowel bleeding (formerly known as obscure bleeding) with refractory faecal evacuation disorder. She underwent a radionuclide scan which picked up Meckel’s Diverticulum (MD) (Figure 1A). Her anorectal manometry demonstrated paradoxical Recto-Anal Inhibitory Reflex (RAIR) suggestive of HD [2]. Barium defecography was also suggestive of HD (Figure 1B).
HD is often associated with other intestinal (4%) diseases like pyloric stenosis, intestinal atresia, and MD [3]. It should be suspected in younger patients with unexplained gastrointestinal bleeding and constipation.
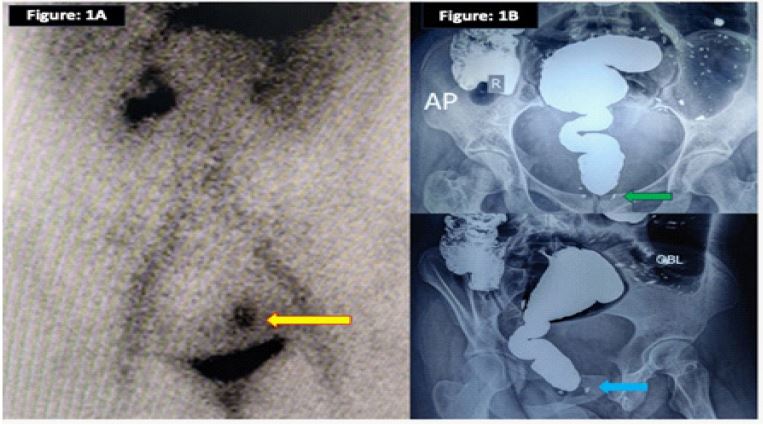
Figure 1B: Barium defecography showing dilated rectosigmoid region with abrupt tapering which corresponds to the aganglionic zone. This is suggestive of Hirschsprung disease.
References
- Amiel J, Sproat-Emison E, Garcia-Barcelo M, et al. Hirschsprung disease, associated syndromes and genetics: A review. J Med Genet. 2008; 45: 1-14.
- Tran VQ, Mahler T, Bontems P, et al. Interest of anorectal manometry during long-term follow-up of patients operated on for Hirschsprung’s disease. J Neurogastroenterol Motil. 2018; 24: 70-8.
- Sy ED, Shan YS, Yang YR, et al. Hirschsprung’s disease, a rare precipitating factor in neonatal perforated Meckel’s diverticulum. J Pediatr Surg. 2006; 41: 1319-21.