
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Co-infection invasive pulmonary aspergillosis and pneumocystis jiroveci infection in B-cell acute lymphoblastic leukemia
Thiraporn Kanjanaphan*; Ruaywan Suntiwes; Wirapatra Iamwat; Daranee Isaranimitkul; Supreeya Padungsak
Department of Pediatrics, Faculty of Medicine, Vajira Hospital, Navamindradhiraj University, Thailand.
*Corresponding Author : Thiraporn Kanjanaphan
Department of Pediatrics, Faculty of Medicine, Vajira Hospital, Navamindradhiraj university, Thailand.
Tel: +66955192942;
Email: thiraporn@nmu.ac.th
Received : Dec 27, 2023
Accepted : Jan 16, 2024
Published : Jan 23, 2024
Archived : www.jcimcr.org
Copyright : © Kanjanaphan T (2024).
Citation: Kanjanaphan T, Suntiwes R, Iamwat W, Isaranimitkul D, Padungsak S. Co-infection invasive pulmonary aspergillosis and pneumocystis jiroveci infection in B-cell acute lymphoblastic leukemia. J Clin Images Med Case Rep. 2024; 5(1): 2814.
Description
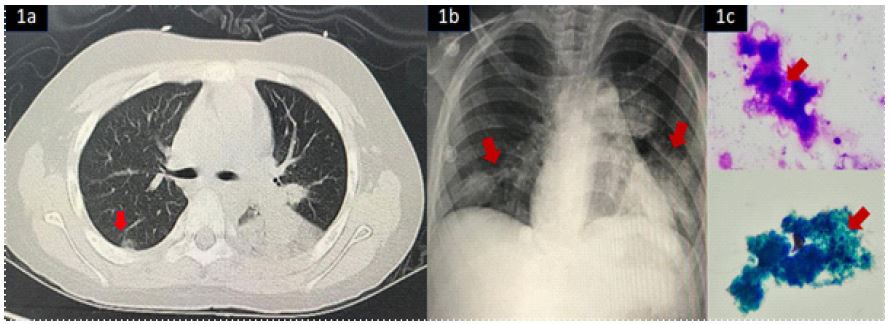
An 8-year-old Thai boy presented with a two-week history of anemia, abnormal purpura in both legs, and was diagnosed with B-cell acute lymphoblastic leukemia (B-cell ALL). Following Thai-POG guidelines, he underwent chemotherapy and received trimethoprim-sulfamethoxazole prophylaxis. However, he developed febrile neutropenia and, despite initial treatment with intravenous meropenem and amikacin, showed no improvement. After a week of febrile neutropenia, a chest CT scan revealed multiple lung nodules (Figure1a). Bronchoalveolar lavage confirmed a positive galactomannan level (1.12 ng/mL). The patient received voriconazole with therapeutic drug monitoring (level: 4.7 ug/mL). Despite this, he experienced progressive dyspnea and hypoxia, and a chest X-ray revealed bilateral ground glass appearance in the lower lungs (Figure 1b). Sputum analysis detected Pneumocystis Jirovecii Pneumonia (PJP) (Figure 1c). Treatment included trimethoprim-sulfonamides, prednisolone, and voriconazole. Within two days, the patient’s symptoms improved. Treatment duration for PJP was 21 days, followed by continued trimethoprim-sulfonamides prophylaxis. Voriconazole was maintained until resolution confirmed by imaging (approximately 6 months). The clinical manifestations of aspergillus infection vary, including ABPA, aspergilloma, chronic aspergillosis, and invasive aspergillosis [1]. Neutropenia duration correlates with the risk of invasive pulmonary aspergillosis [2]. Pneumocystis jirovecii is an opportunistic pathogen, affecting about 12% of children with acute lymphocytic leukemia [3]. A British study reported a 7% annual increase in PJP cases, deaths, and hospital admissions in England from 2000 to 2010 [4]. Both IPA and PJP pose significant threats to immunocompromised children. Although coinfection is rare, this case underscores the importance of a multidisciplinary approach, timely identification, and appropriate interventions for successful outcomes.
Declarations of competing interest: The authors have no competing interests to declare.
Funding statement: Not applicable.
Ethical approval and patient consent statement: Ethics approval and consent from Institutional Review Board Faculty of Medicine Vajira Hospital (COE:020/2023X).
References
- William JS. Aspergillus Species In: Sarah SL, ed. Principles and Practice of Pediatric Infectious Diseases, sixth edition. Philadelphia: Elsevier. 2023; 1262-8.
- Schwartz RS, Mackintosh FR, Schrier SL, Greenberg PL. Multivariate analysis of factors associated with invasive fungal disease during remission induction therapy for acute myelogenous leukemia. Cancer. 1984; 53: 411-9.
- Burke BA, Good RA. Pneumocystis carinii infection. Medicine. 1992; 71: 165-75.
- Maini R, Henderson KL, Sheridan EA, Lamagni T, Nichols G, et al. Increasing Pneumocystis Pneumonia, England, UK, 2000-2010. Emerg. Infect. Dis. 2013; 19: 386-92.