
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Co-infection of toxoplasma and blastocystis sp. in a CKD patient with SLE background: A case report
Bahareh Razmand1*; Danial Touzandehjani2
1Parasitology and Mycology Department, Medicine Faculty, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2Immunology Department, Medicine Faculty, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
*Corresponding Author : Bahareh Razmand
Parasitology and Mycology Department, Medicine Faculty, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Email: baharraz1991@gmail.com
Received : Oct 20, 2023
Accepted : Jan 17, 2024
Published : Jan 24, 2024
Archived : www.jcimcr.org
Copyright : © Razmand B (2024).
Abstract
Toxoplasma and Blastocystis sp. are two common single-celled parasites found worldwide. Although the pathogenesis of Blastocystis sp. is still unknown, it is frequently reported in immunocompromised patients. Toxoplasmosis is also becoming a primary health concern due to its high occurrence rate globally. Parasitic coinfections are rare but can occur in individuals with weakened immune systems. Parasites have adapted mechanisms to evade innate and cellular immunity, which can result in immune system dysfunction and an increased risk of coinfections. Patients undergoing dialysis for end-stage chronic kidney disease are particularly at risk of infections due to immune system dysregulation. Chronic infections can also lead to increased immune complexes that include complements. Dysregulation of complement system proteins such as C3 and C4 can cause host tissue failures in patients with autoimmune disorders. This case report presents the first documented case of a coinfection of Toxoplasmosis and Blastocystis infection in a chronic kidney disease patient with systemic lupus erythematosus background.
Keywords: Toxoplasmosis; Blastocystis sp; Co-infection; Complement System; End-stage chronic kidney disease.
Abbreviations: CKD: Chronic kidney disease; SLE: Systemic lupus erythematosus; ESRD: End-stage renal disease; HUS: Hemolytic uremic syndrome.
Citation: Razmand B, Touzandehjani D. Co-infection of toxoplasma and blastocystis sp. in a CKD patient with SLE background: A case report. J Clin Images Med Case Rep. 2024; 5(1): 2815.
Introduction
Toxoplasma gondii, an intracellular parasite, can infect various warm-blooded animals, including humans. Toxoplasmosis can cause severe complications, including ocular and cerebral Toxoplasmosis, in people with compromised immune systems. Transmission of the parasite is possible through consuming undercooked meat, contaminated water, or contact with infected cat feces. Evaluation of antibodies against the parasite is the method used to diagnose Toxoplasmosis [1].
Blastocystis sp. is a single-celled parasite found in the intestines of humans and various animals. It is one of the most common human parasites, with a global prevalence rate. While it is considered a normal part of the human gut microbiota in some cases, it can also cause gastrointestinal symptoms such as diarrhea, abdominal pain, and bloating. Blastocystis infection has also been associated with immune-related disorders and chronic gastrointestinal symptoms. Diagnosis is typically made through stool samples; treatment options include antimicrobial medications and probiotics [2].
Toxoplasmosis and Blastocystis infection are parasitic infections that can cause significant inflammations in susceptible individuals directly or through immune responses. The activation of the complement system and eosinophilia can result in the deposition of immune complexes, particularly in organs like the brain, eye, lungs, or kidney, caused by both infections. The immune responses to the parasites can lead to the deposition of immune complexes, which in the long term can cause eosinophilic nephritis, leading to kidney inflammation and failure. CKD patients with weakened immune systems are more susceptible to infections. Therefore, kidney failure patients must avoid contact with potentially contaminated environments, practice proper hygiene, and seek prompt medical attention if any symptoms suggestive of parasitic infection arise [3,4].
Case presentation
A 24-year-old female with end-stage chronic kidney disease visited a private nephrology medical center in Tehran in September 2023. She was referred due to complaints of fatigue, abdominal pain, and diarrhea. The patient’s medical history revealed undergoing SLE treatment with Hydrocortisone and weekly dialysis sessions. After evaluating her symptoms, the physician ordered routine laboratory examinations for the patient.
Blood samples were collected for a Complete Blood Count (CBC), Erythrocyte Sedimentation Rate (ESR), and quantitative C-reactive protein (CRP). A CRP level of 7.1 mg/l (normal range up to 6) and ESR 18 mm/h. (Normal range 0-15) were estimated through blood examination. The patient’s CBC found a likely unknown allergic reaction due to increased eosinophil count (Table 1).
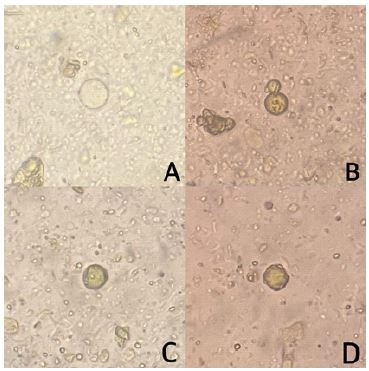
The physician recommended that the patient undergo further examination at the laboratory due to eosinophilia, abdominal complications, and a history of contact with domestic animals. To investigate parasitic infections, the laboratory conducted stool examination, blood tests, including Toxoplasma IgM and IgG. An inflammatory panel consisting of complement components and enzymatic markers was also carried out during the blood examination. The microscopic observation of the stool sample revealed a positive test for Blastocystis sp. (Figure 1). The complete results of the laboratory examination showed a chronic inflammatory profile (Table 2).
Higher-than-normal C3 levels indicated an infection. Based on Toxoplasma IgG and positive stool exam for Blastocystis sp., the patient was diagnosed with chronic Toxoplasmosis and Blastocystis infection. To control parasitic infection and inflammation, the patient went under anti-parasitic medications, including oral Metronidazole 500 mg/ 12h, oral Trimethoprim/sulfamethoxazole 400 mg/ 80 mg/ 12h, and anti-inflammatory therapy. The patient was not admitted to the hospital and was asked to follow up weekly to investigate the inflammatory reduction.
Table 1: The complete blood count result (performed by Mindray analyzer BC-5500 and approved by microscopic differentiation).
| Test | Result | Unit | Normal Range |
|---|---|---|---|
| WBC | 9.13 | 10^3/ µl | 4.0-10.0 |
| RBC | 3.95 | 10^6/ µl | 4.2-5.4 |
| HGB | 10.1 | g/dl | 11.0-15.0 |
| PLT | 244 | 10^3/ µl | 140-440 |
| Neutrophils | 64.7 | % | 50-70 |
| Lymphocytes | 25.1 | % | 20-40 |
| Eosinophils | 11.2 | % | 0.0-5.0 |
Table 2: The results of laboratory investigations.
| Test | Result | Unit | Method | Normal Range |
|---|---|---|---|---|
| Toxoplasma IgG | 88.1 | IU/ml | ELISA | Negative <9 Borderline 9-11 Positive >11 |
| Toxoplasma IgM | 0.1 | IU/ml | ELISA | Negative <0.9 Borderline 0.9-0.11 Positive >0.11 |
| IgE | 72 | IU/ml | EIA | 10-100 |
| C3 | 138.1 | mg/dl | Turbidimetric | 75-135 |
| C4 | 30.7 | mg/dl | Turbidimetric | 9-36 |
| LDH | 401 | U/L | - | Up to 500 |
| CPK | 132 | U/L | - | Up to 160 |
| SGOT | 30 | U/L | - | Up to 31 |
| SGPT | 42 | U/L | - | Up to 32 |
Discussion
Despite being competitive, parasitic infections can occur concurrently and chronically in rare cases. The presence of simultaneous infections on a long-term basis will lead to an overstimulation of the immune system, including the complement system, and chronic eosinophilia, which will then lead to immune suppression. As a result of this reduced immunity, new infections will have a better chance to occur. Additionally, long-term chronic parasitic infections such as Toxoplasmosis can lead to immune system dysregulation, affecting the complement system, leading to impaired immune function and increased susceptibility to other infections. The complement system can be evaded by parasites, leading to chronic infections with severe long-term consequences [5-7].
The complement system is a network of proteins that eliminate pathogens. There are three pathways to activate it: classical, lectin, and alternative. The classical pathway is triggered when antibodies attach to the surface of pathogens, while the lectin pathway is activated when lectin or ficolins attach to specific carbohydrates. The alternative pathway is always active and can be triggered by microbes lacking complement inhibitors. C3 breakdown generates small amounts of C3b, which bind to the pathogen surface and initiate MAC formation, causing cell lysis [8].s
The complement system is essential for maintaining health, but any abnormalities in it can cause harm to tissues and organs and even lead to death. Autoimmune disorders and parasitic infections, among other causes, can result in complement dysregulation. For instance, Toxoplasma renders C3 ineffective in evading the complement system, which leads to chronic activation and tissue damage. Understanding this dysregulation is crucial for preventing further tissue damage in patients with autoimmune disorders. Complement regulatory proteins must tightly regulate complement activation to prevent damage to host tissues. Complement dysregulation in patients with SLE or HUS can lead to cardiovascular and dialysis-related complications and increased infection vulnerability [9].
Hemodialysis is a vital treatment for ESRD or CKD patients. Chronic inflammation from CKD can activate the complement system, leading to complement dysregulation. Hemodialysis patients are more susceptible to infections and have altered immune function. The dialysis procedure itself can activate the complement system, releasing pro-inflammatory cytokines and immune cell recruitment, causing an inflammatory response [10].
In this case, we are facing a unique situation where a patient with CKD has both Blastocystis infection and chronic Toxoplasmosis for the first time. Despite receiving treatment for systemic lupus erythematosus, which is meant to reduce complement components, the patient still exhibits a high level of C3. This suggests that the Blastocystis sp. might be causing an infection. Although Blastocystis sp. is known to be a gut microbia and commensal parasite, it can cause abdominal complications in immunocompromised patients.
During the treatment of SLE, there is a decrease in C3 levels, which could be reversed in case of concurrent infections. Therefore, chronic infections or immunosuppressants can easily stimulate new infections, including microbiome infections. Chronic parasitic infections that last for unknown periods cause immune system dysregulation. The relationship between suppressed immunity and complement dysregulation in chronic infections is bidirectional. The chronic suppression caused by parasitic infection through eosinophilia and complement activation speeds up tissue damage, particularly in patients with weakened immune systems. This loop of immunity dysregulation caused by chronic infections continues to cause new infecinfections and cell damage, such as kidney failure.
Conclusion
The complement system is an essential part of the immune system that plays a crucial role in host defense against pathogens such as parasites. Toxoplasmosis and Blastocystis infection, leading to significant inflammation via complement system activation or eosinophilia. Understanding parasitic infections is crucial for developing effective treatment strategies to prevent or mitigate the risk of further damage in CKD patients undergoing dialysis and immunosuppressants treatment.
Declarations
Data availability: The data that has been used is confidential.
Disclosure: This case is funded by correspondence as a case report, not research or study.
Consent: Informed patient consent was obtained.
Declaration of interest: The authors declare that there are no conflicts of interest in this work.
References
- Kalmar Z, Sandor AD, Balea A, Borsan SD, Matei IA, et al. Toxoplasma gondii in small mammals in Romania: the influence of host, season and sampling location. BMC Vet Res. 2023; 19(1): 177.
- Engsbro AL, Stensvold CR, Vedel Nielsen H, Bytzer P. Prevalence, incidence, and risk factors of intestinal parasites in Danish primary care patients with irritable bowel syndrome. Scand J Infect Dis. 2014; 46(3): 204-9.
- Jones NJ, Chess J, Cawley S, Phillips AO, Riley SG. Prevalence of risk factors for foot ulceration in a general haemodialysis population. Int Wound J. 2013; 10(6): 683-8.
- Babekir A, Mostafa S, Obeng-Gyasi E. The Association of Toxoplasma gondii IgG Antibody and Chronic Kidney Disease Biomarkers. Microorganisms. 2022; 10(1).
- Xiao J, Li Y, Gressitt KL, He H, Kannan G, et al. Cerebral complement C1q activation in chronic Toxoplasma infection. Brain Behav Immun. 2016; 58: 52-6.
- El Saftawy EA, Amin NM, Hamed DH, Elkazazz A, Adel S. The hidden impact of different Blastocystis genotypes on C-3 and IgE serum levels: A matter of debate in asthmatic Egyptian children. J Parasit Dis. 2019; 43(3):4 43-51.
- Young CR, Yeo FE. Blastocystis and schistosomiasis coinfection in a patient with chronic kidney disease. Case Rep Med. 2014; 2014: 676395.
- Arshad A, Chung W, Isherwood J, Steward W, Metcalfe M, et al. Restoration of mannose-binding lectin complement activity is associated with improved outcome in patients with advanced pancreatic cancer treated with gemcitabine and intravenous omega-3 fish oil. JPEN J Parenter Enteral Nutr. 2014; 38(2): 214-9.
- Afolabi H, Zhang BM, O’Shaughnessy M, Chertow GM, Lafayette R, et al. The Association of Class I and II Human Leukocyte Antigen Serotypes With End-Stage Kidney Disease Due to Membranoproliferative Glomerulonephritis and Dense Deposit Disease. Am J Kidney Dis. 2023.
- Oda T, Yoshizawa N. Factors Affecting the Progression of Infection-Related Glomerulonephritis to Chronic Kidney Disease. Int J Mol Sci. 2021; 22(2).